



A 55-year-old woman with a history of hypertension was admitted to our institution due to severe dyspnea. On physical examination tachypnea, hypotension, and bilateral jugular distension were detected. The electrocardiogram showed sinus tachycardia. Chest radiography revealed mild bilateral pleural effusions and severe cardiomegaly (Figure 1A). An echocardiogram showed a 3-cm global pericardial effusion with signs of cardiac tamponade (Figure 1B). Due to the patient's clinical instability, drainage of the pericardial effusion was mandatory, but pericardiocentesis was unsuccessful due to catheter obstruction, and so surgical drainage was performed through a pleuropericardial window. Cytology and pericardial biopsy detected no malignant cells. Abdominal computed tomography showed ascites and a 3 cm × 4 cm ovarian fibroma (Figure 1C). Given the benign nature of the tumor, an expectant attitude was adopted.
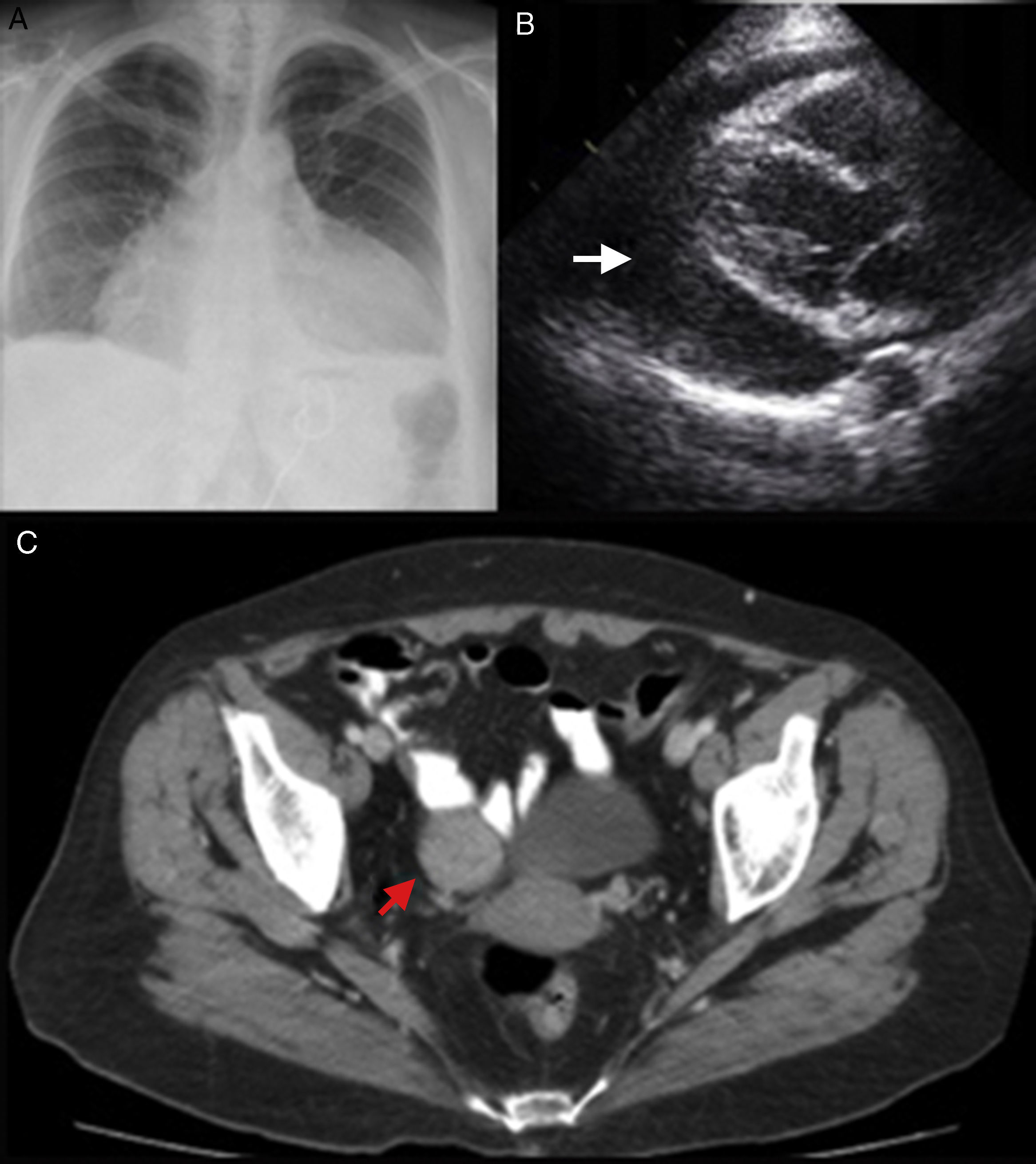
A: Anteroposterior chest X-ray showing mild bilateral pleural effusion and massive bottle-shaped heart manifesting severe cardiomegaly; B: Two-dimensional echocardiography showing a 3-cm global pericardial effusion (arrow) and signs of cardiac tamponade; C: Pelvic computed tomography showing a right ovarian tumor, a fibroma (arrow).
The triad of ascites, hydrothorax and a benign ovarian tumor defines a rare clinical entity termed Meigs syndrome. However, ascites and hydrothorax have been also reported in the presence of tumors located in the uterus, tubes or colon. Such variants have been termed pseudo-Meigs syndrome.1–3 Subsequently a new variant appeared, known as Meigs-like syndrome,4 which associates pericardial effusion with the original definition of Meigs syndrome. The origin of the fluid accumulations is unknown; inflammatory cytokines and hormonal or tumoral stimulation are possible etiologies.5 Dyspnea, jugular distension and hypotension suggest the presence of pericardial effusion and cardiac tamponade is its acute presentation. The diagnosis is confirmed by echocardiography and pericardial drainage is indicated. An abdominal CT scan can confirm the presence of an ovarian tumor. It is mandatory to exclude an ovarian tumor in any woman with unexplained pericardial effusion.4
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
