



A 71-year-old man underwent a Bentall procedure a year ago; his medical history was negative for any immunosuppressive conditions. Eight months later, he was admitted with a history of high fever (38.6°C). Blood cultures were drawn on arrival, which identified Trichosporon inkin, treated with intravenous amphotericin B. A subsequent transesophageal echocardiogram revealed a hypermobile vegetation attached to the valve causing severe flow obstruction (Figure 1). Urgent surgery was performed.
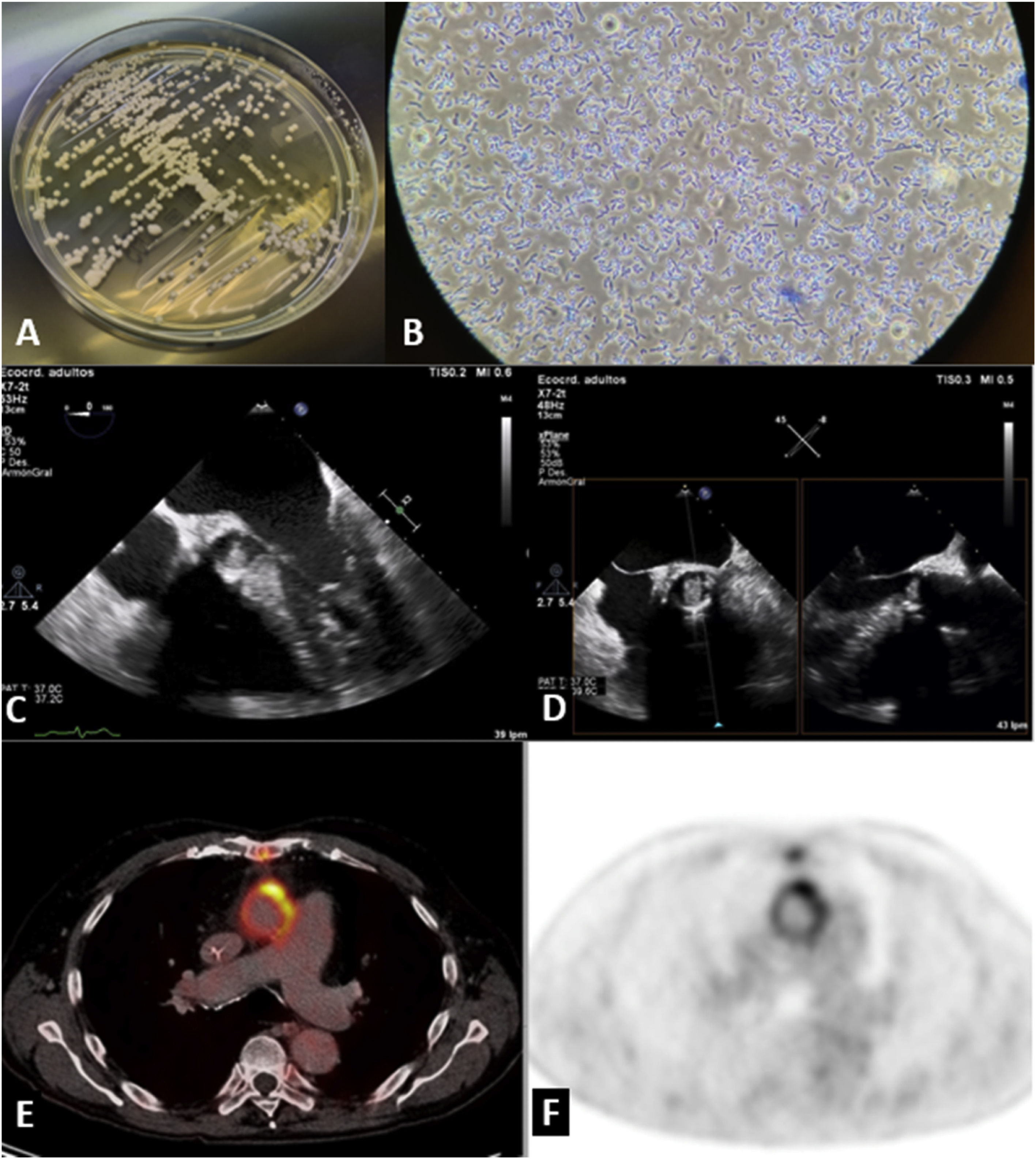
(A) Trichosporon inkin: Sabouraud glucose agar, 30°C, 7 days; (B) T. inkin arthroconidia and blastoconidia (lactophenol cotton blue 40×); (C) transesophageal echocardiogram showing a hypermobile mass causing severe obstruction (D and E) at the aortic valve; (E) positron emission tomography fused with computed tomography with a maximum standardized uptake value of 13 showing a vegetation located in the left anterolateral aortic wall.
Five months later, positron emission tomography fused with computed tomography (PET/CT), performed due to persistent fever, confirmed a peritubular relapse of the T. inkin infection, requiring urgent surgery and redo of the Bentall procedure, without further complications. This time, the vegetation was attached to the Dacron tube.
An immunological study was performed, with no remarkable findings. The patient was discharged on 200 mg fluconazole daily guided by antifungal susceptibility testing, without relapse since then.
Conflicts of interestThe authors have no conflicts of interest to declare.
