




Coronary fistulas are rare malformations with an estimated incidence of <1% in angiographic studies. They are usually diagnosed as incidental findings on coronary angiography. Detection by echocardiography is rarely reported; the most frequent finding is right chamber dilatation, as in most cases the fistula drains directly into the right heart.
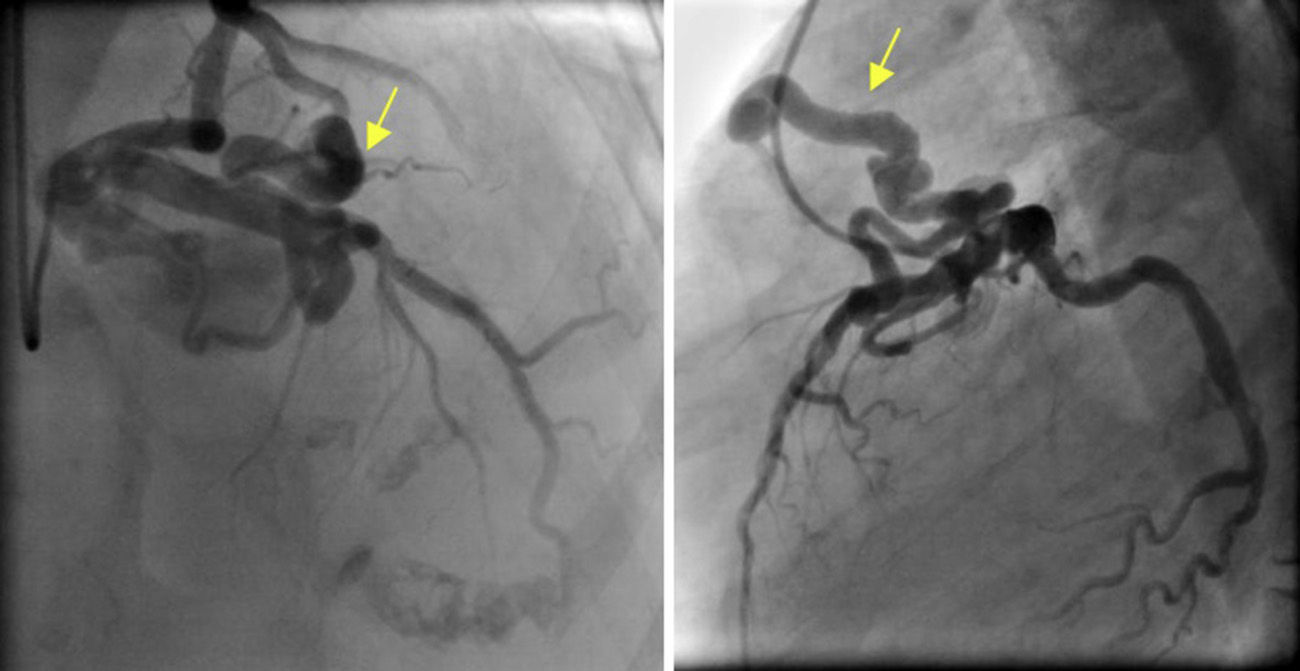
A 66-year-old woman with permanent atrial fibrillation was admitted for fatigue on moderate exertion. On physical examination, a systolic-diastolic murmur was detected at the left sternal border. She had previously undergone transthoracic echocardiography, which showed normal-sized cardiac chambers, good biventricular function and no significant valve disease. Coronary angiography revealed no angiographic lesions but identified a large coronary fistula arising from the proximal segment of the anterior descending artery and draining into the pulmonary artery (Figure 1), causing a left-to-right shunt.
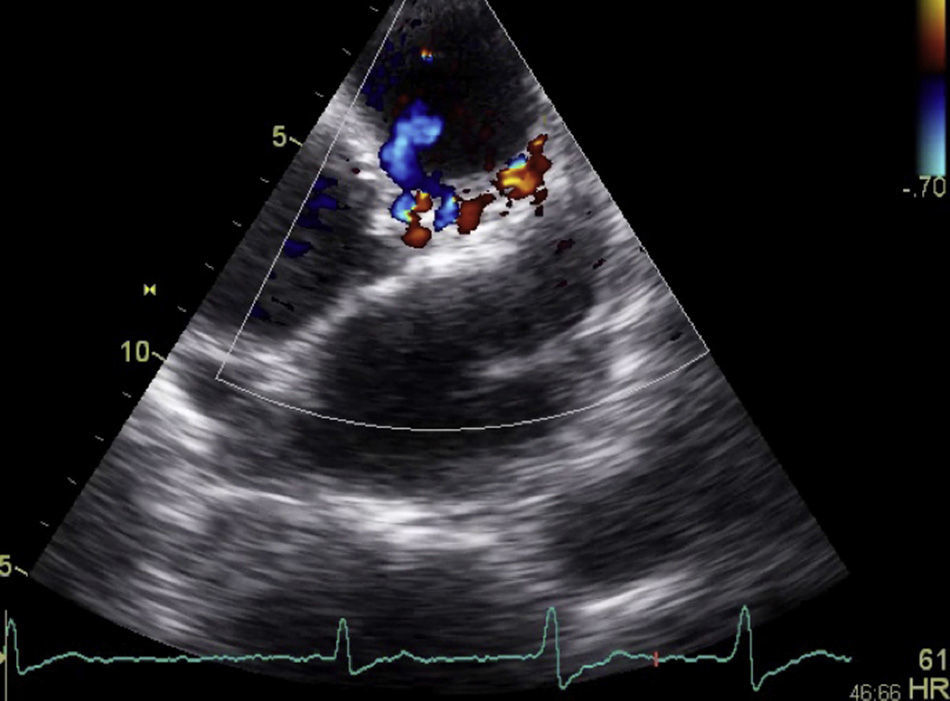
Further echocardiographic assessment in parasternal view documented dilatation of the pulmonary artery trunk (34 mm) and normal-sized right chambers. Doppler echocardiography identified continuous laminar flow, mainly in diastole, peak velocity 0.1 m/s (Figure 2), corresponding to the site of coronary fistula drainage. Areas of turbulent flow were seen along the course of the anterior descending artery, corresponding to branching of the fistula at this point (Figure 3). Pulmonary artery pressure was estimated at 28 mmHg. No other congenital defects were detected.
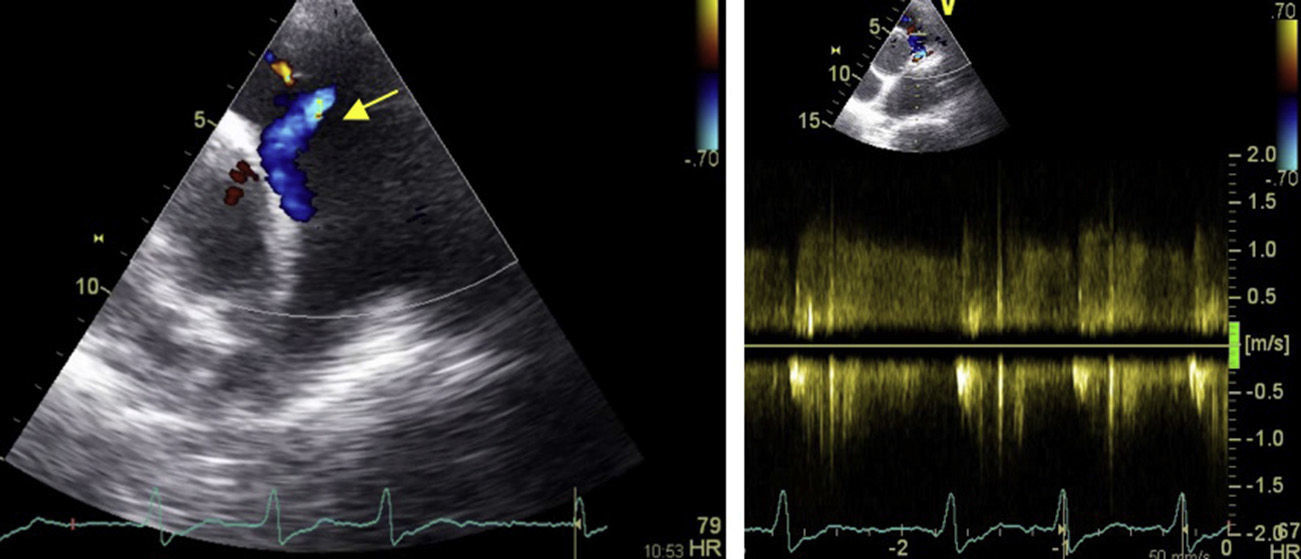
Transthoracic echocardiogram, parasternal short-axis view. Left: color Doppler showing laminar flow draining into the proximal portion of the pulmonary artery trunk (yellow arrow), as well as slight pulmonary regurgitation; right: continuous Doppler revealing the flow to be systolic-diastolic (mainly diastolic), with peak velocity of 1.0 m/s.
Since the patient was symptomatic, it was decided to perform percutaneous closure, but this was unsuccessful and she subsequently underwent surgical ligation of the fistula.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Almeida I, Caetano F, Trigo J, et al. O ecocardiograma transtorácico no diagnóstico de uma fístula coronária. Rev Port Cardiol. 2014;33:655–656.
