




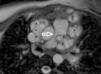
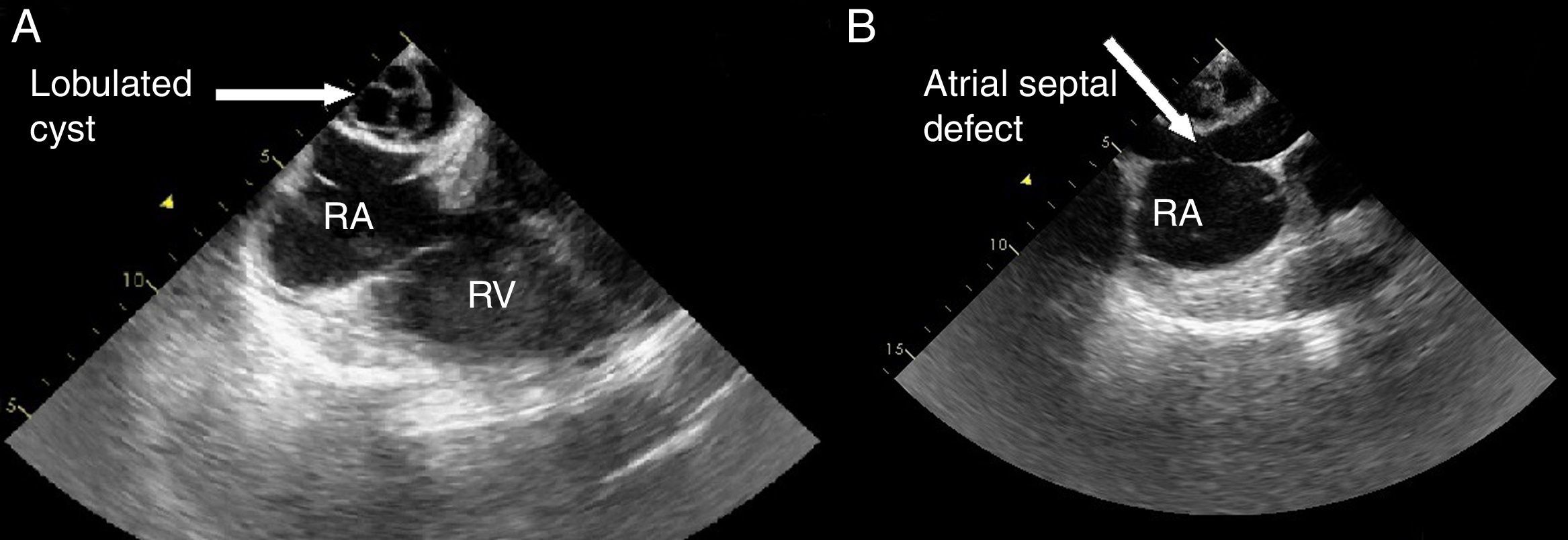
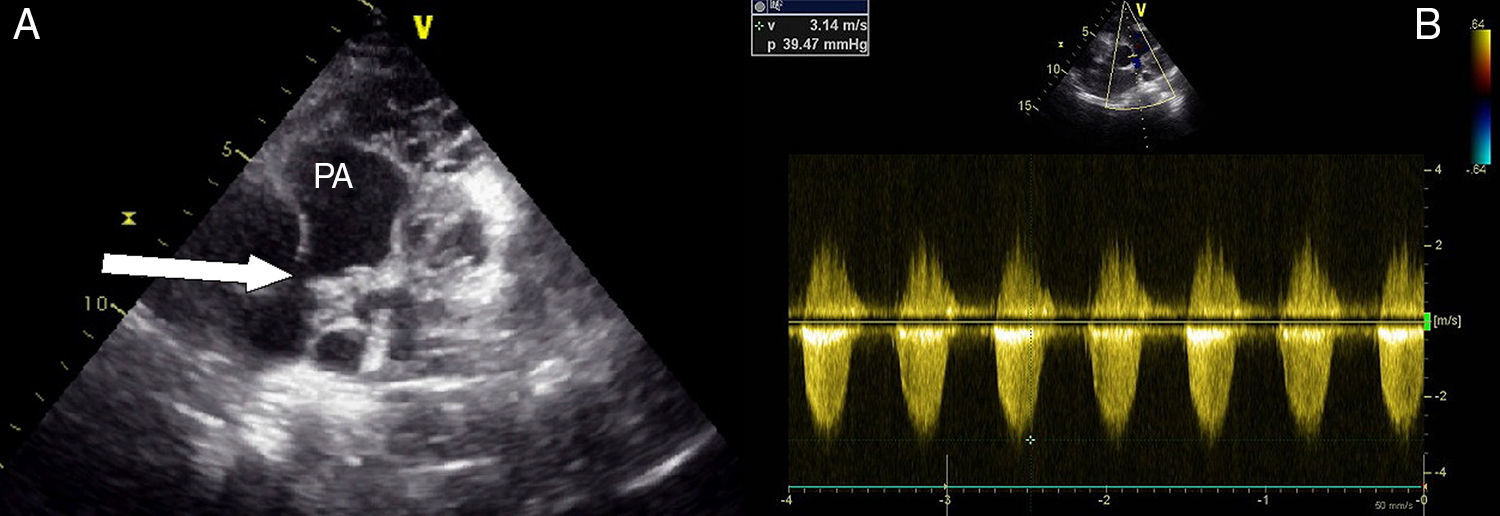
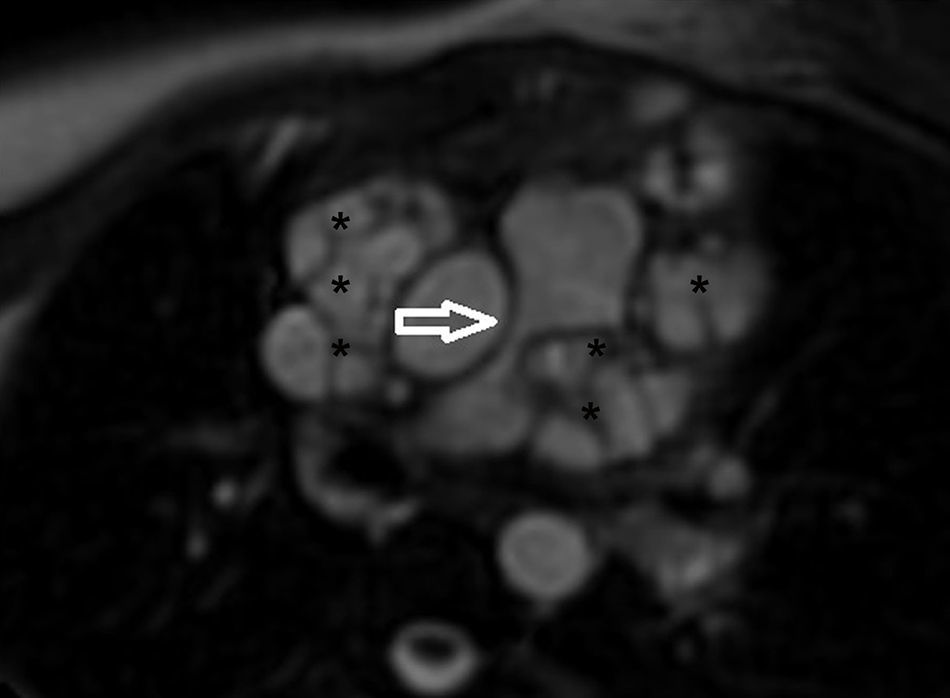
A 21-year-old woman was admitted to our clinic with dyspnea. Her medical history was unremarkable. Right bundle branch block was identified on 12-lead ECG and mediastinal enlargement on the chest X-ray. Transthoracic and transesophageal echocardiographic examination showed a lobulated cystic image in the left atrium and secundum-type atrial septal defect (Figures 1 and 2). Additionally, in short-axis view a mass was visualized invading the pulmonary artery, and continuous wave Doppler of the pulmonary artery revealed a maximum gradient of 40 mmHg. A detailed examination with cardiac magnetic resonance imaging demonstrated a multicystic mass in the mediastinum compressing the main pulmonary artery, predominantly the left branch (Figure 3). The patient was diagnosed with secundum atrial septal defect and mediastinal hydatid cyst on the basis of serologic tests and detailed history. Surgical therapy was offered and she asked for time to think. Medication with albendazole was started, but she was then lost to follow-up.
Hydatid cyst is a parasitic disease caused by Echinococcus granulosus. The predominantly affected organs are the liver and the lung; mediastinal location is very rare.1 The preferred method for management is surgery but adjunctive albendazole therapy is the subject of debate.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interestThe authors have no conflicts of interest to declare.
