



We report the case of a 70-year-old man with cardiovascular risk factors and a history of a heart murmur diagnosed during infancy, presenting with worsening exertional dyspnea during the previous six months. The physical examination showed a slow-rising carotid pulse, a grade III/VI mid-systolic murmur, crepitant rales on pulmonary auscultation and peripheral edema. Laboratory tests revealed a normal complete blood count, plasma brain natriuretic peptide level of 2500 pg/ml, normal levels of ionized calcium and phosphate and normal renal function. Echocardiographic study showed concentric left ventricular (LV) hypertrophy with preserved ejection fraction, mild diastolic dysfunction (impaired relaxation) and severe aortic valve stenosis with a valve area of 0.6 cm2/m2. Calcified masses were also observed in the mid-LV cavity on 2D and 3D echocardiography (Figure 1A and B, arrows; Videos 1 and 2), causing turbulent flow depicted by color Doppler (Figure 1C; Video 3). Steady-state free precession cine cardiac magnetic resonance (CMR) confirmed the presence of a transversely arranged membrane, suggestive of an anomalous, abnormally thickened and calcified band (Figure 1D and E, arrowheads; Video 4). This non-obstructive structure was connected to the anterolateral papillary muscle and the lateral LV wall by multiple fibrous filaments. The presence of fibrosis was excluded by late gadolinium enhancement CMR.
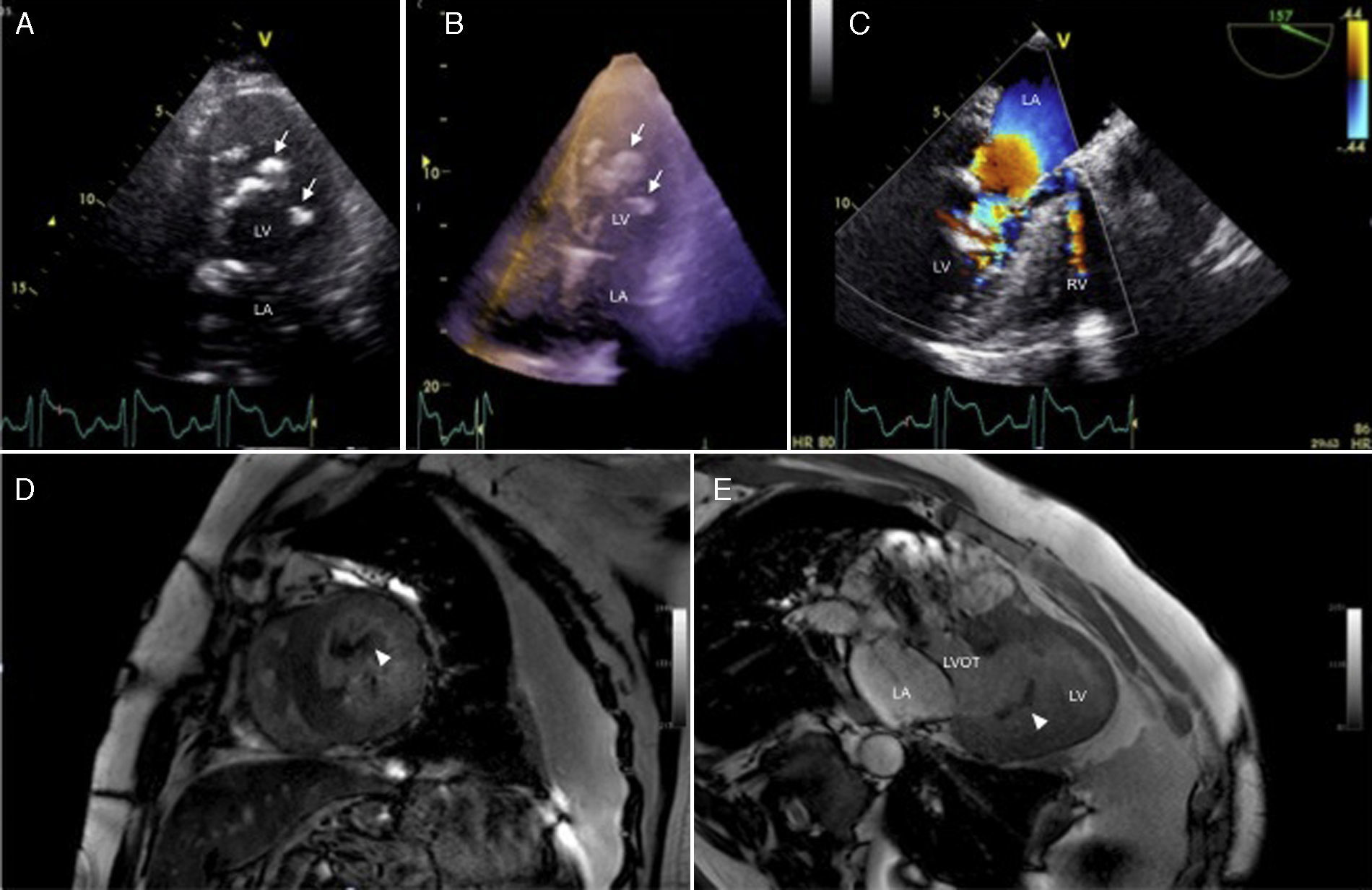
(A) Two-dimensional transthoracic echocardiography, apical 4-chamber view, showing several nodular hyperechogenic masses with acoustic shadowing in the mid-left ventricular cavity (arrows); (B) three-dimensional transthoracic echocardiography, left ventricular full-volume view depicting all of the nodular masses within the left ventricular cavity (arrows); (C) two-dimensional Doppler color flow transesophageal echocardiography, mid-esophageal 3-chamber view with turbulent flow across the mid-left ventricular cavity; (D and E) steady-state free precession cine cardiac magnetic resonance, short-axis and 3-chamber long-axis views with a hypointense linear structure inside the left ventricle (arrowheads). LA: left atrium; LV: left ventricle; LVOT: left ventricular outflow tract; RV: right ventricle.
LV false tendons are fibromuscular structures of varying length and thickness that traverse the ventricular cavity and are accepted as anatomic variants. Calcium deposits in the heart are common in older persons and have been described in association with coronary artery disease, dilated cardiomyopathy, aorto-mitral valvular disease and renal disease. We report a case of massive left ventricular false tendon calcification associated with aortic valve calcification and stenosis.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interestThe authors have no conflicts of interest to declare.
