



Monitoring complex congenital heart disease patients in specialized centers using magnetic resonance (MR) imaging is recommended to prevent late complications. 3D imaging techniques provide better spatial comprehension; however, fully automatic recognition in these patients is difficult. To improve this, the authors propose semi-automatic individual chamber segmentation created from a contrast-enhanced MR angiography. As examples, a heart with no structural pathology and two common surgical procedures are shown in Figure 1.
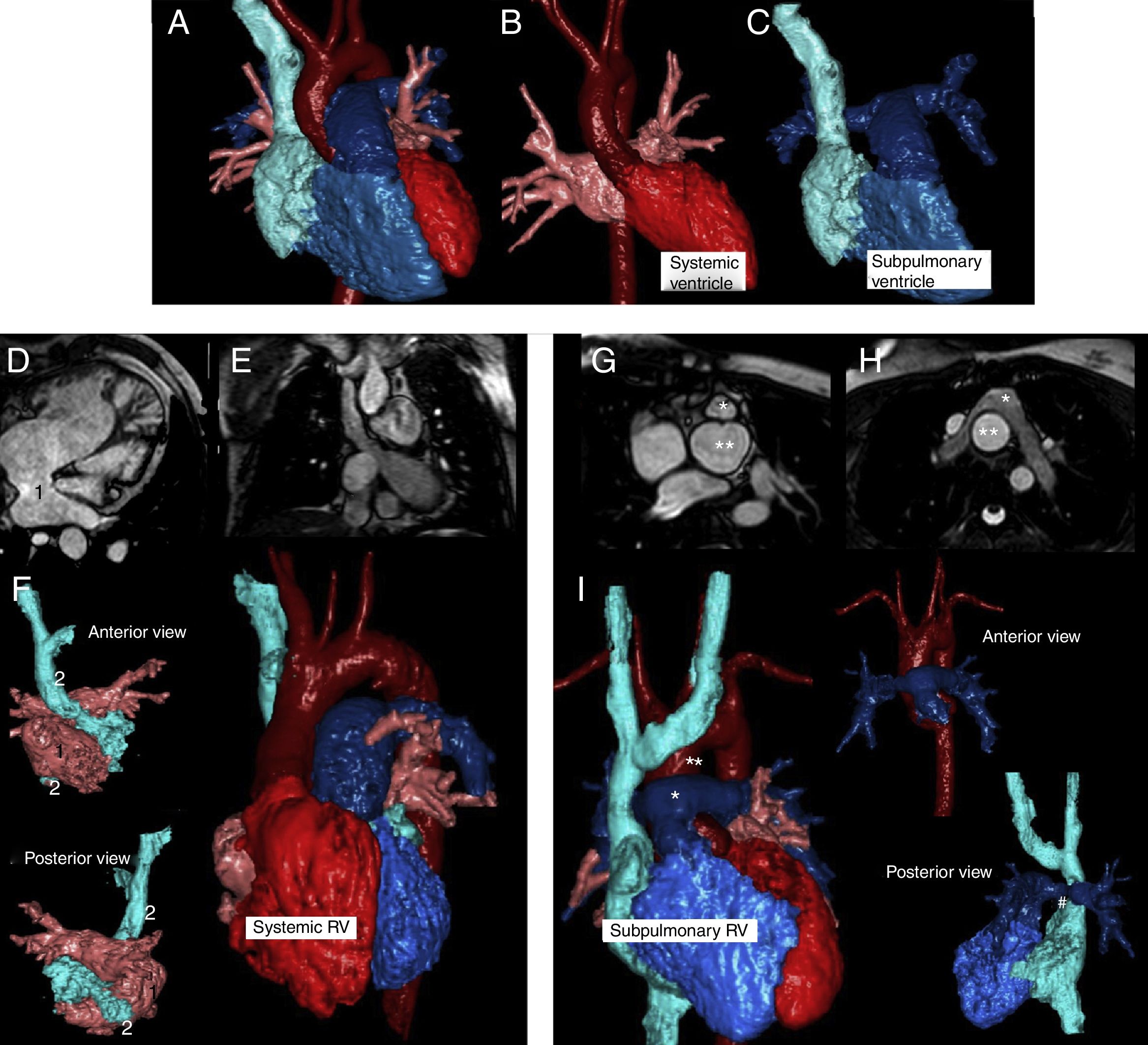
Normal heart (A-C). Chambers are color-coded; systemic chambers are red and subpulmonary chambers are blue. Atria baffles are indicated in images D to F (1, systemic baffle. 2, subpulmonary baffle. Image F, anterior and posterior view of both atria. Note the right ventricle as systemic on the whole heart rendering). In arterial switching, the abnormal position of the great vessel can be seen in images G to I (*: pulmonary artery. **: aortic root. Image I, anterior position of pulmonary artery and a subpulmonary right ventricle. Upper right, anterior view of great vessels and below, a posterior view of the subpulmonary chambers. Note the right pulmonary branch narrowing (#) between the ascending aorta and the superior vena cava).
Each cardiac chamber has been independently processed as individual volume with commercial software (CT Viewer, Philips Healthcare). The whole heart imaging is the sum of each volume, so the user could remove or include any volume individually. This approach may be especially interesting for educational purposes. The additional value could be better noted on videos included as supplementary material.
As a brief summary, children born with complete transposition of great arteries due to atrioventricular concordance and ventriculoarterial discordance (L-TGA) need surgical correction during early childhood. In the atrial switch procedure, blood is redirected in the atrium using a baffle. Blood from pulmonary veins is redirected through the tricuspid valve into the subaortic morphologic right ventricle and blood from systemic drainage is diverted to the subpulmonary morphologic left ventricle through the mitral valve, leaving the morphologic right ventricle as a systemic pump. Conversely, in the arterial switch procedure, blood is redirected in the great vessels by switching the pulmonary artery to an anterior position with principal pulmonary branches enclosing the ascending aorta, thereby restoring ventriculoarterial concordance.
Conflicts of interestThe authors have no conflicts of interest to declare.
The following are the supplementary material to this article:
Normal heart (Video 1). Note the sequential selection of different chambers to show anatomical or relationship findings. The same methodology is shown in a patient with atrium switch (Video 2) and in a patient with arterial switch (Video 3).
