









Estimates of the burden of ischemic heart disease (IHD), including geographic differences, should support health policy decisions. We set out to estimate the burden of IHD in mainland Portugal in 2013 by calculating disability-adjusted life years (DALYs) and to compare this burden between five regions.
MethodsYears of life lost (YLLs) were calculated by multiplying the number of IHD deaths in 2013 (Statistics Portugal) by the life expectancy at the age at which death occurred. Years lived with disability (YLDs) were computed as the number of cases of acute coronary syndrome, stable angina and ischemic heart failure multiplied by an average disability weight. Crude and age-standardized DALYs (direct method, Standard European Population) were calculated for mainland Portugal and for the Northern, Central, Lisbon, Alentejo and Algarve regions.
ResultsIn 2013, 95413 DALYs were lost in mainland Portugal due to IHD. YLLs accounted for 88.3% of the disease burden. Age-standardized DALY rates per 1000 population were higher in men than in women, across the entire country (8.9 in men; 3.4 in women) and within each region, ranging from 7.3 in the Northern and Central regions to 11.8 in the Algarve in men, and from 2.6 in the Northern region to 4.6 in Lisbon in women.
ConclusionsNearly 100000 DALYs were lost to IHD in Portugal, mostly through early mortality. This study enables accurate comparisons with other countries and between regions; however, it highlights the need for population-based studies to obtain specific data on morbidity.
A carga de doença atribuível à doença isquémica do coração (DIC), nomeadamente possíveis diferenças regionais, deve orientar políticas de saúde. Pretendemos estimar a carga de doença atribuível a DIC em Portugal continental em 2013, através do cálculo dos anos de vida saudável perdidos (DALY) e comparar estas estimativas entre regiões.
MétodosCalcularam-se os anos de vida perdidos (YLL) multiplicando o número de mortes por DIC em 2013 (Instituto Nacional de Estatística) pela esperança média de vida à idade da morte. Estimaram-se os anos vividos com incapacidade (YLD) através do número de casos de síndrome coronária aguda, angina estável e insuficiência cardíaca isquémica. Os DALY brutos e padronizados para a idade (método direto, população-padrão europeia) foram calculados para Portugal continental e para as regiões Norte, Centro, Lisboa, Alentejo e Algarve.
ResultadosEm 2013, perderam-se 95 413 DALY em Portugal por DIC. Destes, 88,3% foram por morte prematura. A taxa de DALY perdidos por 1000 habitantes padronizada para a idade foi mais elevada nos homens em todo o país (8,9 nos homens; 3,4 nas mulheres) e em cada região, variando de 7,3 no Norte e Centro até 11,8 no Algarve nos homens, e de 2,6 no Norte a 4,6 em Lisboa nas mulheres.
ConclusõesQuase 100 mil DALY foram perdidos em Portugal devido a DIC, essencialmente por mortalidade prematura. Este estudo permite comparar a carga de doença com outros países e entre regiões, salientando-se, no entanto, a necessidade de estudos de base populacional que forneçam informação específica de morbilidade.
Ischemic heart disease (IHD) remains a leading cause of death worldwide.1,2 However, the case-fatality rate of acute myocardial infarction has decreased markedly,3 resulting in a growing population of survivors with disability due to angina, recurrent infarction or ischemic heart failure. Furthermore, the growth and aging of populations means the absolute number of people living with IHD is expected to increase.1
IHD mortality in Portugal has decreased markedly over the last three decades, as in most developed countries.4 Using the IMPACT IHD mortality model, we previously estimated that the proportional contribution to the decline in IHD death of the use of treatments to reduce case fatality, compared to the contribution of favorable risk factor changes, was larger than in other countries.5 This reflects high-quality coverage of sophisticated medical interventions but less effective primary prevention, which also contributes to the prevalence of IHD-related disability in the Portuguese population.
Disability-adjusted life years (DALYs) are a health gap measure that combines both time lost due to premature mortality and non-fatal conditions, and are calculated as the sum of years of life lost (YLLs) due to premature mortality and years lost due to disability (YLDs).6,7 Calculating the burden of IHD is challenging taking into account its different clinical presentations, including myocardial infarction, angina and heart failure, which raises methodological concerns regarding the large amount of information needed and the lack of registries in many countries,8 including Portugal. According to the 2010 Global Burden of Diseases, Injuries and Risk Factors (GBD) study, IHD is one of the top three causes of DALYs in Portugal, along with low back pain and cerebrovascular disease,9 but without estimates of absolute DALYs, YLLs and YLDs numbers, ranking positions alone do not enable results to be compared between countries, and more detailed and updated information are required.
Previous reports on mortality time trends and global estimates of the burden of disease due to IHD in Portugal have considered overall national data. However, there is considerable variability within the country in rates of mortality and hospital admissions of patients with IHD, possibly reflecting differences in economic and social development and urbanization.10 This variability can be expected to impact access to health care and the efficiency of the health system in dealing with IHD, and if differences are found in DALYs across regions, this may support a readjustment of recommendations and allocation of healthcare resources.
Therefore, our aim was to estimate the burden of IHD in mainland Portugal in 2013 by calculating DALYs and to compare this burden between five regions of the country: North, Central, Lisbon, Alentejo and Algarve.
MethodsBased on the GBD 2010 study,11 we calculated the burden of IHD, considering that it may result in death or three general clinical presentations: acute coronary syndrome (myocardial infarction and unstable angina), stable angina, and ischemic heart failure. GBD studies prior to 2010 used a 3% discount rate and age weights that placed the greatest emphasis on health outcomes in young adults, but in the GBD 2010 study, DALYs were simplified and in the present analysis, no discount factors or weighting by age were applied.1
DALYs were calculated for each gender and age group (<40, 40-49, 50-59, 60-69, 70-79, and ≥80 years) and by region of mainland Portugal (Nomenclature of Territorial Units for Statistics [NUTS] II: Northern, Central, Lisbon, Alentejo, Algarve) that included 9918548 inhabitants in 2013.12 Similar procedures and data sources were adopted to compute DALYs for Portugal and for the five national regions considered for analysis. All sources of information are summarized in Table 1.
Sources of information for each of the parameters used to calculate disability-adjusted life years lost due to ischemic heart disease in mainland Portugal, 2013.
| Parameter | Information source |
|---|---|
| Population data | INE |
| Deaths due to IHD | INE |
| Standard life expectancy | GBD 2010 |
| Incidence of acute coronary syndrome episodes in 2013 | ACSS |
| Prevalence of stable angina episodes | OFRECE study |
| Distribution of stable angina by severity | AVANCE registry |
| Prevalence of HF | PRICE study |
| Distribution of HF by etiology | GALICAP study |
| Distribution of HF by severity | GALICAP study |
| Disability weights | GBD 2013 |
ACSS: Administração Central do Sistema de Saúde (Central Administration of the Health System); GBD: Global Burden of Disease Study; HF: heart failure; IHD: ischemic heart disease; INE: Instituto Nacional de Estatística (Statistics Portugal).
YLLs were calculated by multiplying the number of deaths in each age group by the life expectancy at the age at which death occurs.13
Data regarding the number of deaths by IHD in each gender and age group (five-year intervals until ≥85 years) in Portugal and the five regions in 2013 were provided by Statistics Portugal.12 All deaths with International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) codes I20 to I25 were considered.14
The standard life expectancy was provided by the GBD 2010 study. It represents the normative goal of survival and was computed based on the lowest recorded death rates across countries in 2010. Life expectancy at birth is 86.02 years, equal for men and women.13 Since only the total number of deaths by age group was available, mean age at death was set to the mid-point of each five-year age group, except for the oldest group (assumed to be 87.5 years).6 The total of YLLs for each gender was obtained by summing the YLLs of all age groups.
Years lived with disabilityYLDs due to IHD were computed as the number of cases multiplied by an average disability weight for all possible combinations of the clinical presentations (acute coronary syndrome, stable angina and heart failure), taken separately or together (seven possible combinations). For each clinical presentation we used the most up-to-date disability weights provided by the GBD study.15
Specific data on the Portuguese population were used if information was available for the year 2013. If not, we preferentially chose robust population studies carried out in Spain around the year 2013, with data by gender and age groups, given the similarities in patterns of cardiovascular disease between the two Iberian countries.16
Acute coronary syndromeData on numbers of patients admitted to a hospital with myocardial infarction or unstable angina were obtained from the National Hospital Discharge Register, centrally held in the Central Administration of the Health System (ACSS). Episodes were selected in which the main diagnosis was coded as 410 or 411.1 according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). The duration of each episode of acute coronary syndrome was set at 28 days, in accordance with the GBD 2010 study,17 with the first two days presenting a higher disability weight. This information was used to calculate the prevalence of this clinical presentation.
Stable anginaNo national studies reporting the prevalence of stable angina were identified, therefore we used estimates from the OFRECE study conducted between 2010 and 2012, which reports the prevalence of confirmed angina by gender and age group in a representative sample of the Spanish population aged 40 years or older.18 Three levels of stable angina were considered according to severity (mild, moderate or severe), each was assigned a specific disability weight and the proportions of angina cases were obtained from the AVANCE registry.19 The disability weight for angina is the weighted average of these specific disability weights.
Heart failureNo population-based studies reporting the prevalence of heart failure in Portugal contained data collected more recently than 1998,20 which we believe made it impossible to provide a credible scenario of the epidemiology of heart failure in 2013. We therefore used data from the Spanish PRICE study conducted between 2004 and 2005.21 Only ischemic heart failure was considered, and the proportion of heart failure cases with ischemic etiology was obtained from the GALICAP study conducted in a representative sample of Galicia (northern Spain) (36.8% in men and 26.6% in women).22 From the same study, we obtained information concerning the severity of heart failure, classified according to New York Heart Association functional class.23 The disability weight for ischemic heart failure is the weighted average of mild, moderate and severe specific disability weights.
Calculation of average disability weights and prevalence of ischemic heart diseaseAssuming that disability in patients with multiple clinical presentations increases but is less than the sum of individual disability weights, an average disability weight for IHD was computed for each of the seven possible combinations among all clinical manifestations (only acute coronary syndrome, only angina, only ischemic heart failure, acute coronary syndrome and angina, acute coronary syndrome and ischemic heart failure, angina and ischemic heart failure, acute coronary syndrome and angina and ischemic heart failure), according to the multiplicative adjustment method.24
Regarding the overlap of different clinical presentations, the overall prevalence of IHD is lower than the sum of prevalences of each diagnosis. The probability of overlap was estimated assuming independence between diseases24 and this proportion was subtracted to avoid double counting of cases. By multiplying the estimated prevalence of each combination by the resident population in Portugal in 2013 in each gender and age group, we obtained the number of cases, which was then multiplied by the average disability weight. To obtain the final YLDs for each gender, we summed the YLDs contributed by all seven combinations.
Age-standardized DALYs per 1000 population were calculated using the direct method and were adjusted to the Standard European Population.25
ResultsPopulation size and number of cases in mainland Portugal in 2013 for each of the clinical manifestations used for calculation of DALYs are presented in Table 2.
Population size, number of deaths and number of cases of acute coronary syndrome, stable angina and ischemic heart failure, by age group and gender in mainland Portugal, 2013.
| Men | Women | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Populationa | No. of deathsb | ACS casesc | Angina casesd | HF casese | Populationa | No. of deathsb | ACS casesc | Angina casesd | HF casese | |
| Age group | ||||||||||
| <40 years | 2227791 | 24 | 144 | 0 | 0 | 2226603 | 6 | 34 | 0 | 0 |
| 40-49 years | 711832 | 111 | 713 | 2249 | 3587 | 765955 | 19 | 188 | 1612 | 2573 |
| 50-59 years | 653478 | 288 | 1598 | 10279 | 10970 | 716378 | 60 | 379 | 4511 | 4800 |
| 60-69 years | 541945 | 533 | 1787 | 4506 | 14923 | 630779 | 188 | 694 | 4596 | 10828 |
| 70-79 years | 380495 | 916 | 1744 | 17667 | 16326 | 503468 | 550 | 1100 | 21990 | 17548 |
| ≥80 years | 198787 | 1612 | 1257 | 5925 | 11729 | 361037 | 2219 | 1535 | 7842 | 16290 |
| Total | 4714328 | 3484 | 7243 | 40627 | 57536 | 5204220 | 3042 | 3930 | 40551 | 52039 |
ACS: acute coronary syndrome; HF: heart failure.
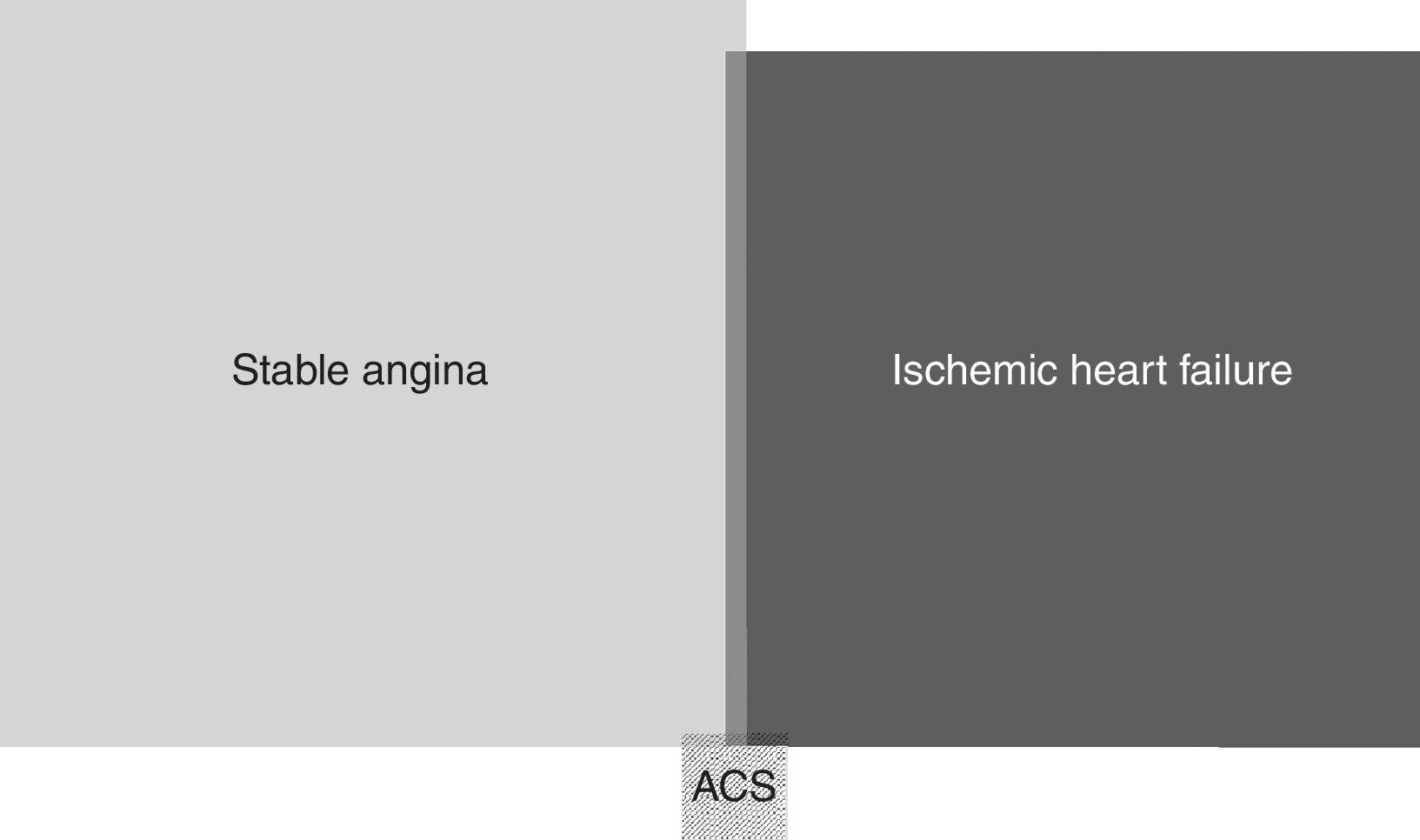
In 2013, 95413 DALYs were lost in mainland Portugal due to IHD (58689 in men; 36724 in women), which corresponds to 9.6 DALYs per 1000 population (12.4 in men; 7.0 in women). The age-adjusted DALY rate was 6.0 per 1000 population (8.9 in men; 3.4 in women). The age-adjusted YLL rate per 1000 population was 8.1 and 2.8 in men and women, respectively, which accounted for 88% of the disease burden (90% in men; 85% in women). The proportional contributions of acute coronary syndrome, stable angina and ischemic heart failure to YLDs are shown in Figure 1, with angina and heart failure being the main contributors, due to their chronic nature.
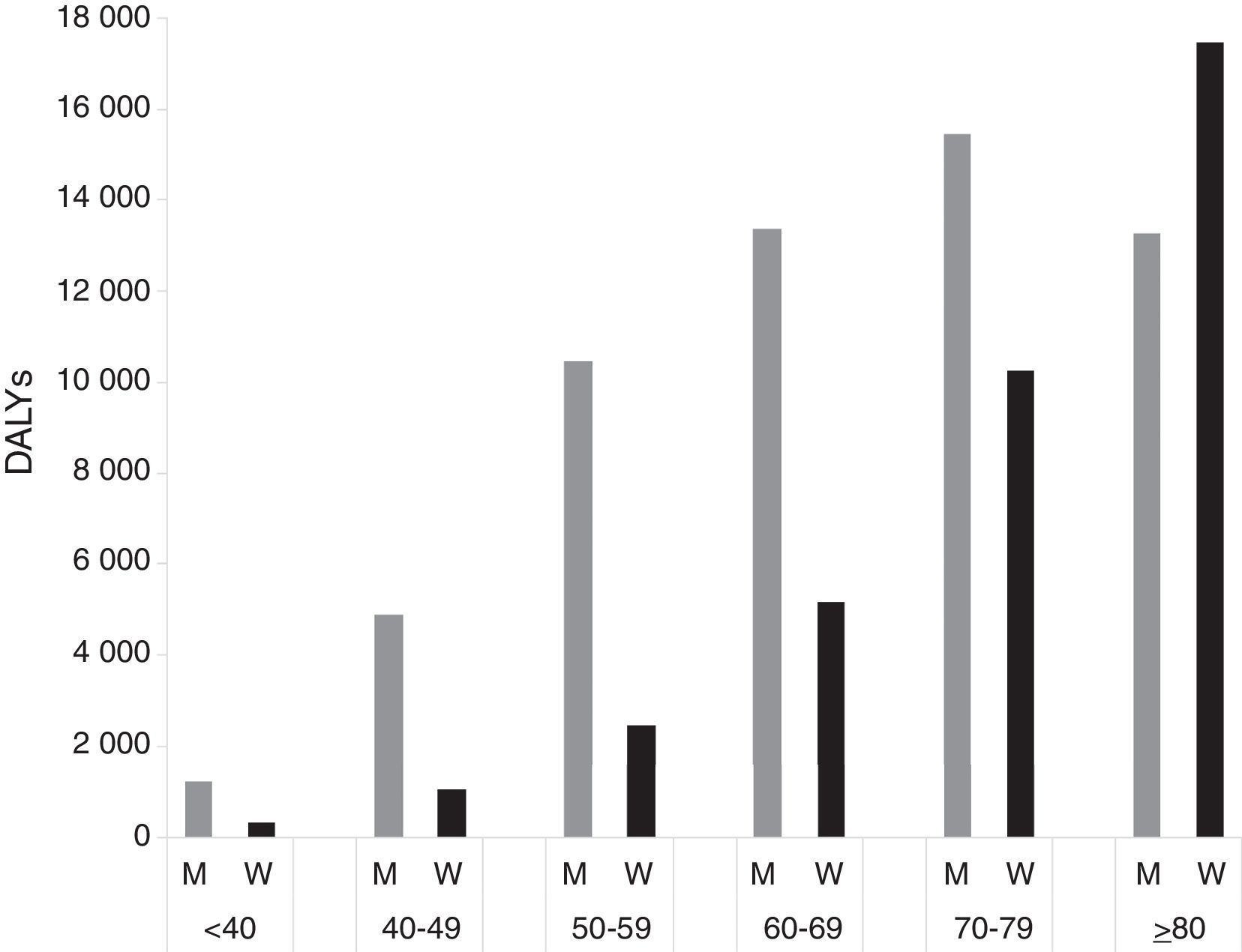
The absolute number of DALYs was higher in men than in women in every age group except those aged 80 years or over. In men, the highest burden of IHD was observed in the 70-79 age group, accounting for 15440 DALYs, while in women the highest number of DALYs was observed in the oldest group (≥80 years: 17466) (Figure 2 and Table 3). Considering DALYs per 1000 population, the burden was highest in men and women aged at least 80 years (66.8 and 48.4, respectively) (Table 3).
Years lived with disability, years of life lost due to premature mortality and disability-adjusted life years in mainland Portugal, by NUTS II region, age and gender, 2013.
| Men | Women | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| YLD | YLL | DALYs | YLL/DALYs | DALYs/1000 population | YLD | YLL | DALYs | YLL/DALYs | DALYs/1000 population | |
| Portugal | ||||||||||
| <40 years | 1.10 | 1227 | 1228 | 1.00 | 0.55 | 0.55 | 316 | 317 | 1.00 | 0.14 |
| 40-49 years | 329 | 4563 | 4892 | 0.93 | 6.87 | 242 | 787 | 1030 | 0.76 | 1.34 |
| 50-59 years | 1251 | 9217 | 10469 | 0.88 | 16.02 | 563 | 1912 | 2475 | 0.77 | 3.45 |
| 60-69 years | 1021 | 12366 | 13387 | 0.92 | 24.70 | 870 | 4297 | 5167 | 0.83 | 8.19 |
| 70-79 years | 2061 | 13380 | 15440 | 0.87 | 40.58 | 2471 | 7799 | 10270 | 0.76 | 20.4 |
| ≥80 years | 986 | 12286 | 13272 | 0.93 | 66.77 | 1391 | 16075 | 17466 | 0.92 | 48.4 |
| Total | 5649 | 53039 | 58689 | 0.90 | 12.45 | 5537 | 31187 | 36724 | 0.85 | 7.06 |
| Northern | ||||||||||
| <40 years | 0.48 | 408 | 409 | 100 | 0.49 | 0.23 | 49.1 | 49.3 | 1.00 | 0.06 |
| 40-49 years | 126 | 1442 | 1569 | 0.92 | 5.74 | 94.3 | 78.9 | 173 | 0.46 | 0.58 |
| 50-59 years | 483 | 2254 | 2738 | 0.82 | 10.86 | 217 | 454 | 670 | 0.68 | 2.43 |
| 60-69 years | 361 | 3485 | 3846 | 0.91 | 20.12 | 305 | 1292 | 1597 | 0.81 | 7.22 |
| 70-79 years | 668 | 4100 | 4768 | 0.86 | 38.70 | 810 | 1911 | 2721 | 0.70 | 16.50 |
| ≥80 years | 306 | 2864 | 3171 | 0.90 | 51.30 | 437.26 | 3570 | 4007 | 0.89 | 35.27 |
| Total | 1946 | 14554 | 16500 | 0.88 | 9.50 | 1862.92 | 7355 | 9218 | 0.80 | 4.83 |
| Central | ||||||||||
| <40 years | 0.33 | 200 | 200 | 1.00 | 0.41 | 0.13 | 107 | 107 | 1.00 | 0.22 |
| 40-49 years | 74.4 | 483 | 557 | 0.87 | 3.47 | 54.7 | 256 | 310 | 0.82 | 1.81 |
| 50-59 years | 298 | 1708 | 2006 | 0.85 | 12.93 | 131 | 315 | 446 | 0.71 | 2.68 |
| 60-69 years | 242 | 2676 | 2919 | 0.92 | 22.80 | 204 | 649 | 853 | 0.76 | 5.79 |
| 70-79 years | 536 | 2719 | 3255 | 0.84 | 32.91 | 644 | 1822 | 2466 | 0.74 | 18.83 |
| ≥80 years | 278 | 2996 | 3274 | 0.91 | 58.46 | 384 | 3435 | 3819 | 0.90 | 38.31 |
| Total | 1429 | 10782 | 12212 | 0.88 | 11.27 | 1418 | 6583 | 8001 | 0.82 | 6.68 |
| Lisbon | ||||||||||
| <40 years | 0.06 | 405 | 405 | 1.00 | 0.63 | 0.06 | 107 | 107 | 1.00 | 0.16 |
| 40-49 years | 89.1 | 1846 | 1935 | 0.95 | 9.94 | 663 | 369 | 436 | 0.85 | 2.06 |
| 50-59 years | 318 | 3655 | 3973 | 0.92 | 23.81 | 150 | 724 | 875 | 0.83 | 4.56 |
| 60-69 years | 292 | 4117 | 4410 | 0.93 | 28.19 | 259 | 1665 | 1925 | 0.87 | 10.17 |
| 70-79 years | 573 | 4331 | 4904 | 0.88 | 46.17 | 683 | 2905 | 3587 | 0.81 | 25.70 |
| ≥80 years | 245 | 4508 | 4752 | 0.95 | 95.94 | 373 | 6411 | 6784 | 0.95 | 69.84 |
| Total | 1517 | 18862 | 20380 | 0.93 | 15.43 | 1531 | 1218 | 13713 | 0.89 | 9.23 |
| Alentejo | ||||||||||
| <40 years | 0.19 | 102 | 102 | 1.00 | 0.64 | 0.10 | 53.0 | 53.1 | 1.00 | 0.35 |
| 40-49 years | 24.1 | 541 | 565 | 0.96 | 10.90 | 16.4 | 39.4 | 55.9 | 0.71 | 1.08 |
| 50-59 years | 97.8 | 907 | 1005 | 0.90 | 19.77 | 41.1 | 164 | 205 | 0.80 | 3.96 |
| 60-69 years | 79.8 | 1188 | 1267 | 0.94 | 30.07 | 65.1 | 411 | 476 | 0.86 | 10.15 |
| 70-79 years | 187 | 1625 | 1811 | 0.90 | 52.76 | 228 | 896 | 1124 | 0.80 | 24.29 |
| ≥80 years | 106 | 1440 | 1546 | 0.93 | 72.54 | 134 | 1990 | 2124 | 0.94 | 61.53 |
| Total | 494 | 5803 | 6298 | 0.92 | 17.52 | 485 | 3553 | 4038 | 0.88 | 10.52 |
| Algarve | ||||||||||
| <40 years | 0.04 | 111 | 111 | 1.00 | 1.09 | 0.03 | 0.00 | 0.03 | 0.00 | 000 |
| 40-49 years | 14.6 | 251 | 266 | 0.94 | 8.51 | 10.7 | 44.2 | 54.9 | 0.81 | 164 |
| 50-59 years | 54.6 | 692 | 747 | 0.93 | 26.24 | 23.9 | 255 | 278 | 0.91 | 919 |
| 60-69 years | 46.0 | 900 | 946 | 0.95 | 39.09 | 36.5 | 280 | 316 | 0.88 | 1203 |
| 70-79 years | 96.9 | 605 | 702 | 0.86 | 39.34 | 107 | 265 | 372 | 0.71 | 1712 |
| ≥80 years | 50.4 | 478 | 529 | 0.90 | 52.25 | 62.5 | 670 | 732 | 0.91 | 4548 |
| Total | 263 | 3037 | 3300 | 0.92 | 15.44 | 240 | 1513 | 1753 | 0.86 | 7.67 |
DALYs: disability-adjusted life years; YLDs: years lived with disability; YLLs: years of life lost due to premature mortality.
Of the total burden of IHD in men and women, a higher proportional contribution of YLLs was observed in all age and gender groups, with all of the proportions being above 76%. The highest proportional contribution of YLDs was observed in women in the 40-49, 50-59 and 70-79 age groups, accounting for more than 20% of the disease burden (Table 3 and Figure 3).
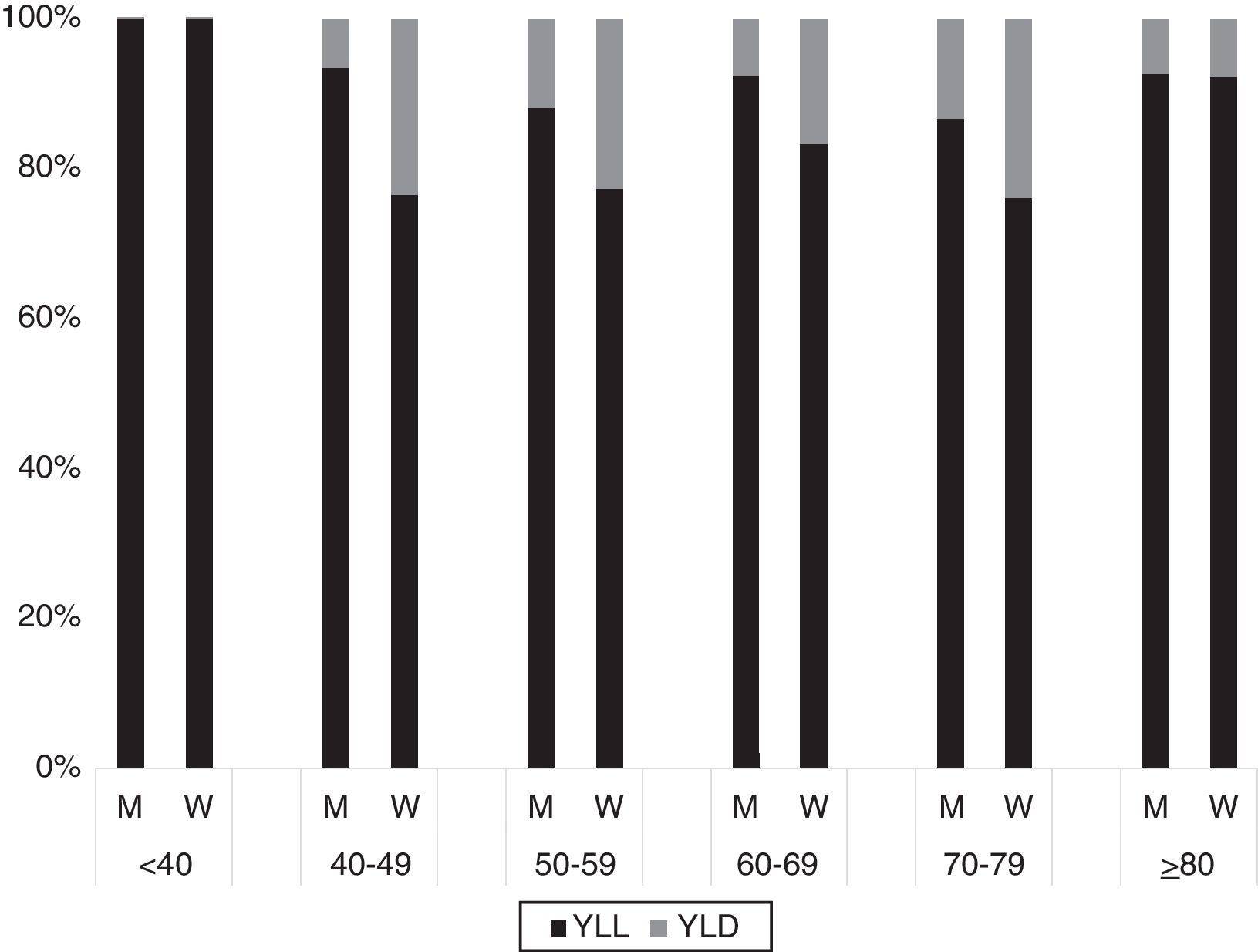
Proportion of years of life lost and years lived with disability in total disability-adjusted life years due to ischemic heart disease by age group and gender in mainland Portugal, 2013. M: men; W: women; YLD: years lived with disability; YLL: years of life lost due to premature mortality.
Table 3 shows the number of YLDs, YLLs and DALYs in the Northern, Central, Lisbon, Alentejo, and Algarve regions and in all of mainland Portugal. Similar patterns of DALYs and their components by age and gender were observed in mainland Portugal and in all five regions, with the oldest age groups presenting the greater burden of IHD and men losing more DALYs due to IHD than women. The absolute number of DALYs was greatest in the Lisbon region (men: 20380; women: 13713) and lowest in the Algarve (men: 3300; women: 1753); however, the highest crude DALY rate per 1000 population was observed in the Alentejo, with 13.9 DALYs lost (17.5 in men and 10.5 in women). The lowest contribution of YLLs in men was found in the Northern region, accounting for 82% of the DALYs in men aged 50-59 years. Concomitantly, the region in which the impact of YLLs was lowest for women was also the Northern, which was the only region with proportions lower than 70% (Table 3).
Figure 4 depicts the age-standardized DALY rate per 1000 population in the Northern, Central, Lisbon, Alentejo and Algarve regions. DALY rates were higher in men than in women within each region across the entire country: in men, they ranged from 7.3 in the Northern and Central regions to 11.8 in the Algarve; in women they ranged from 2.6 in the Northern region and 4.6 in Lisbon. A similar pattern was observed for men and women across the country, with the Northern and Central regions presenting a smaller number of DALYs lost due to IHD compared to the other regions (Figure 4).
Discussion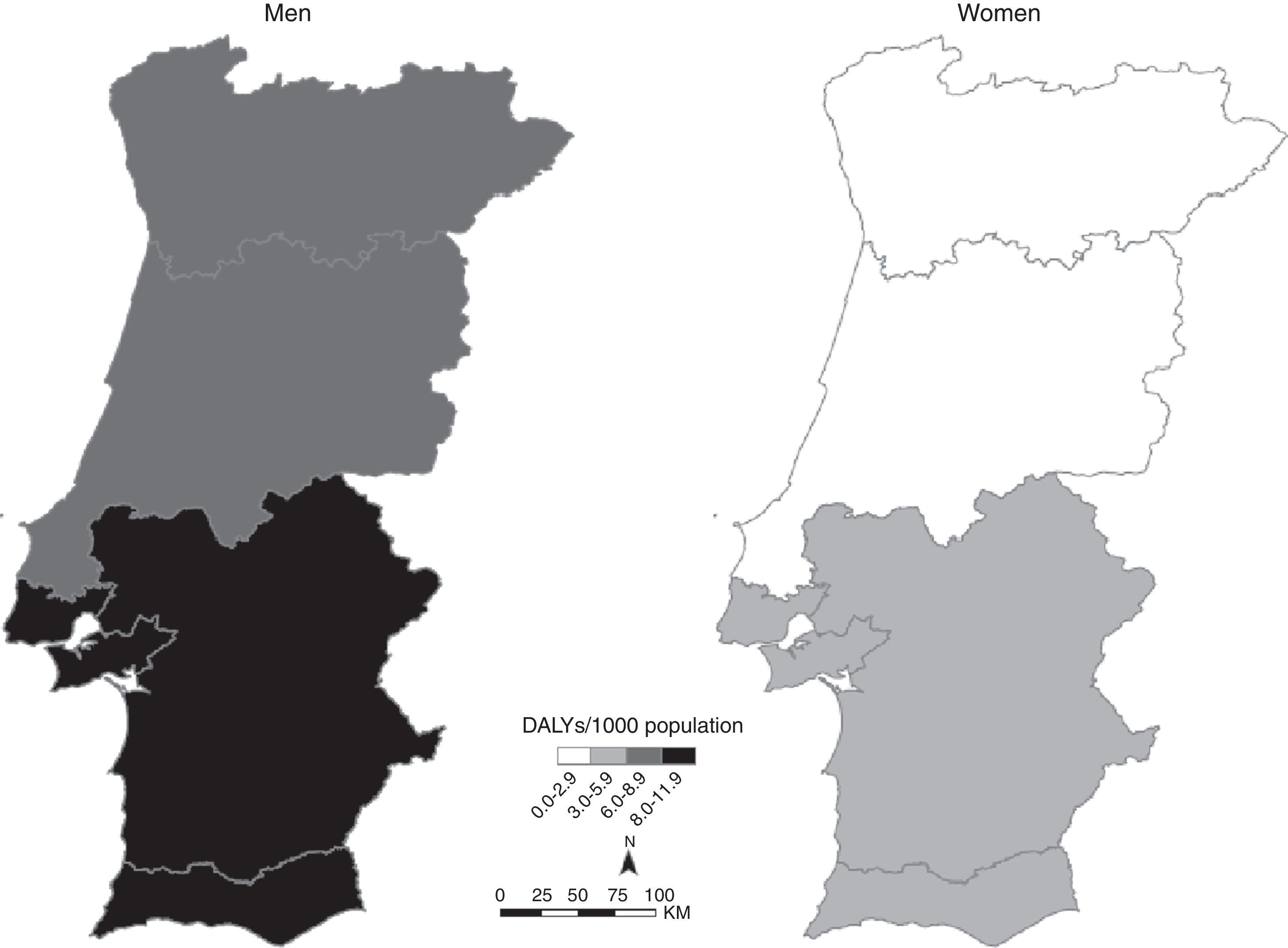
Our results describe the burden of IHD in Portugal through calculation of DALYs, providing information on mortality and disability and pulling together information on acute episodes and chronic expressions of the disease. In 2013, nearly 100000 DALYs were lost due to IHD. Individuals aged over 70 years presented the highest number of DALYs, and the burden was greater in men than in women. YLLs were the major contributors to DALYs lost in both sexes and in almost all age groups. Comparing the different regions of Portugal, despite some regional disparities, similar patterns of DALYs and their components by age and gender were found in men and women, with men presenting a higher age-standardized DALY rate per 1000 population in all regions considered in the analysis.
The age-standardized value of 6.0 DALYs per 1000 population found for Portugal in 2013 is close to the most recent estimates for Spain, in 2008 (8.6).26 Considering data from the GBD 2010 study, the age-standardized rate of DALYs lost in Western Europe due to IHD was 11.6 per 1000 population, and thus our estimates are lower compared to the most recent European results.27
Similarities between the Iberian countries may to some extent be artificial due to the use of the same data sources, particularly for angina and heart failure; however, since the burden of IHD is mainly attributable to mortality, for which we used country-specific data, we believe that this cannot totally explain the similarities between Portugal and Spain. For stable angina and heart failure, we used information from Spain. Although this is a limitation, there are similarities between the two countries in location, socioeconomic and health characteristics.28 No study on angina prevalence using a Portuguese population-based sample was found, but the OFRECE study provided an estimate of prevalences of confirmed angina in a representative sample of Spanish adults.18 Even within Europe, considerable variability is observed, with countries from the north of Europe presenting higher prevalences of angina at least at older ages,29 and so when national data are not available, care needs to be taken to choose estimates from a country that resembles Portugal at least from a health perspective. Concerning heart failure, the EPICA study provides national data on prevalence and severity, based on subjects attending primary health care centers in the community; however, it was conducted in the 1990s.20 The PRICE study, although still well before 2013, is more recent than the EPICA study, to which it bears considerable sociodemographic and methodological similarities. Moreover, the Spanish study provides exact prevalence estimates by age and gender, whereas the Portuguese study only displays them in a chart, requiring an approximate reading. We therefore considered that the more recent Spanish data would be more appropriate.
The use of data from the National Hospital Discharge Register for the number of patients with acute coronary syndrome may have led to an underestimate of the associated YLDs, not only because it includes only inpatients at public hospitals but also because cases that were never hospitalized, particularly those that were asymptomatic or with atypical presentation, may have not been considered. However, the magnitude of this error is expected to be low and without a significant impact in terms of YLDs. Considering the proportion of DALYs attributed to YLLs, the results in the present study are in accordance with the 89% found in Western Europe27 and lower than the 96% found in the Spanish population.26 In 2003-2005, estimates for the Northern region of Portugal attributed 75% of the burden of IHD to YLLs,30 which is lower than the value estimated in this study.
Differences between countries may be partially explained by the use of different data sources and different discount rates and age weighting (2004 GBD methods). Nevertheless, for computation of DALYs in this study, we used the most recent GBD guidelines, which are not age-weighted or discounted over time, in order to facilitate comparisons with recent studies, and we consider that this approach should be used from now on.
At the same time, the lack of up-to-date data regarding the prevalence of stable angina and heart failure is clearly a limitation, since the absence of national data means the analysis may not reflect their prevalence in the Portuguese population. The fact that the severity of these two clinical presentations by region, gender and age group is not specified is also a limitation; it is likely that this lack of precision will mainly affect smaller regions and younger populations, which might result in our results underestimating the differences between strata.
Considering the five different regions of Portugal in this analysis, no substantial differences were found in the patterns of DALYs between men and women, although the age-standardized DALY rate per 1000 population was lower in the Northern and Central regions in both sexes. Although overall living standards have improved, there are disparities in some health indicators (e.g. cancer mortality rates, infant mortality, and number of physicians and nurses per 100000 population), with the Northern region always appearing among the best positions.31 There is no systematic information regarding trends in risk factors by Portuguese regions, but the AMALIA study32 conducted in 2006-2007 showed that the Northern region has a lower prevalence of hypercholesterolemia, hypertension, diabetes and obesity compared to other national regions. If the risk factors for IHD are lower in this region, a lower burden of IHD can also be expected. Moreover, a similar pattern can be found in crude mortality rates due to IHD in Portugal, by gender and region, with men presenting higher rates in each region and the Northern and Central regions presenting a more favorable scenario compared to Lisbon, the Alentejo and the Algarve.33
In this study, YLLs accounted for a higher contribution to the disease burden in men than in women, which is in agreement with higher adjusted mortality and risks attributed to IHD in men observed in other countries.16 Lower IHD mortality among women is most likely explained by their better risk factor profile, even though there is evidence of higher in-hospital mortality after a cardiovascular event and lower access to evidence-based secondary prevention in women compared to men.34 A recent study showed a trend towards smaller gender differences in discharge medications of patients admitted with acute coronary syndromes in Portugal, after adjusting for the potential confounding effects of age, comorbidities and contraindications,35 which is also a possible explanation for the lower burden due to YLLs found among women. Moreover, women tend to adhere more strictly to their doctor's recommendations and to adopt behaviors that will reduce the risk of cardiovascular disease,36 which may contribute to the results found.
ConclusionsThe burden of IHD has a considerable impact on the health of Portuguese adults, particularly in the oldest age groups and mainly in terms of mortality. A regional approach to IHD prevention is needed in order to provide cost-effective interventions for treatment and prevention of IHD.
Our results can be used as a basis to study the burden of IHD in Portugal, using the most recent GBD guidelines. Calculation of DALYs should be conducted periodically in order to analyze changes in this burden over time. This study's systematic and transparent methodology enables accurate comparisons with other countries and between regions within the country; however, it highlights the need for population-based studies to obtain specific data on morbidity and to provide accurate national data by gender, age and region.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interestThe authors have no conflicts of interest to declare.
This project was supported by FEDER funds from Programa Operacional Factores de Competitividade – COMPETE (FCOMP-01-0124-FEDER-028709) and by national funds from the Portuguese Foundation for Science and Technology, Lisbon, Portugal (PTDC/DTP-EPI/0434/2012) and by the Epidemiology Research Unit – Institute of Public Health, University of Porto (UID/DTP/047507/2013).
We would like to thank the Central Administration of the Health System (ACSS) for data from the National Hospital Discharge Register.
