


A 55-year-old male patient, who was a smoker and chronic alcoholic, was admitted to the emergency department with epigastric pain and vomiting which had lasted 14 hours. He had signs of cardiogenic shock. The electrocardiogram showed atrial fibrillation with slow ventricular response and ST-segment elevation in leads II, III, aVF, V1 and V2 (A). Cardiac angiography was performed immediately showing a normal left coronary artery (Figure 1B and C); the right coronary artery (RCA) could not be catheterized. Computed tomography angiography was performed and showed aortic root (AR) and ascending aorta (AA) dilation with diffuse circumferential wall thickening occluding the ostium of the RCA (Figure 1D-F). The wall thickening also extended to the descending aorta (Figure 1D and G). On transesophageal echocardiography, the circumferential thickening of the thoracic aorta had a coarse irregular luminal surface (Figure 1H). The right ventricle was dilated and with severely depressed systolic function (Figure 1I).
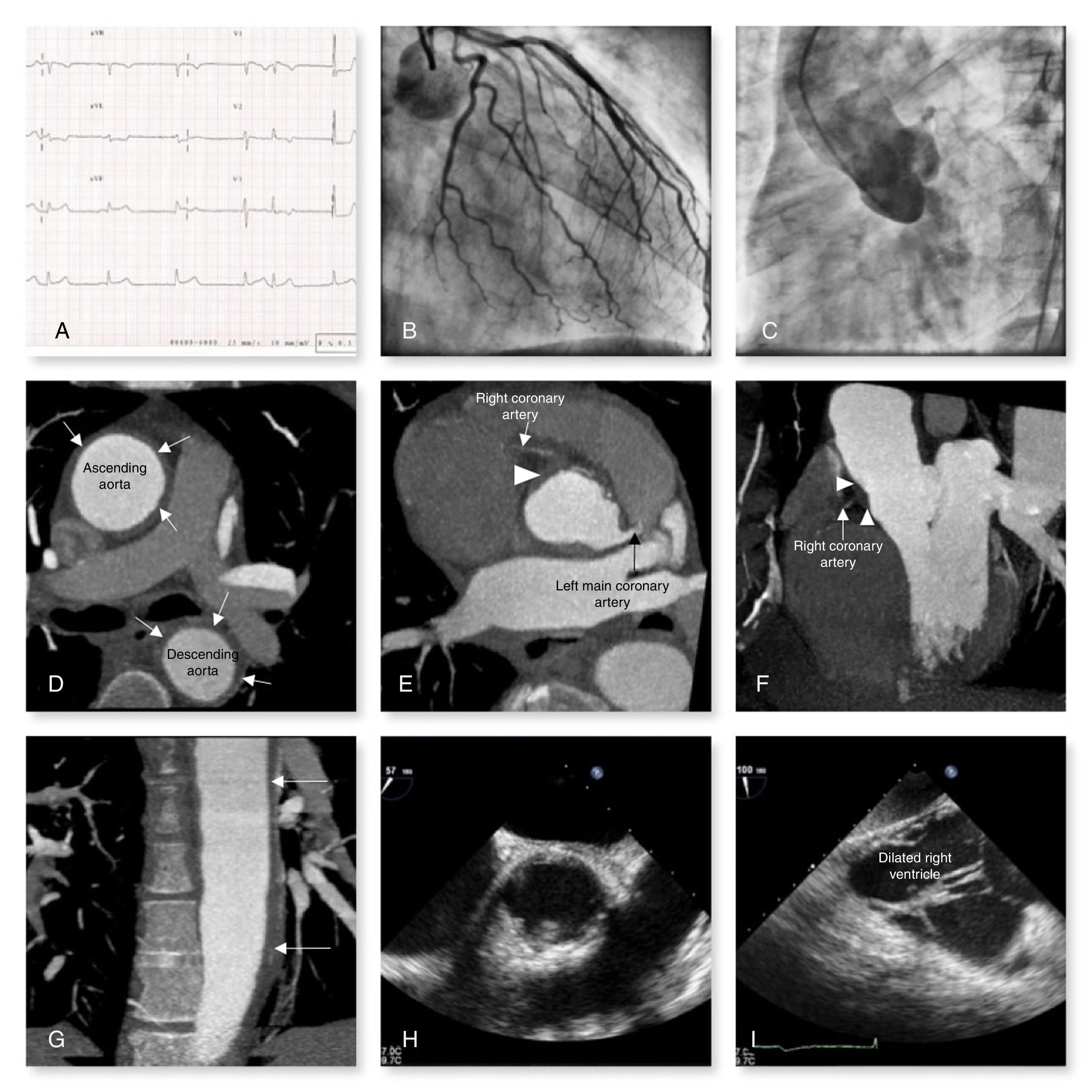
(A) Electrocardiogram on admission; (B) left coronary artery with no atherosclerotic disease; (C) aortography showing mild aortic regurgitation and no signs of ascending aortic dissection; the origin of the left coronary artery can be visualized but the right coronary artery cannot; (D-G) computed tomography angiography showing circumferential wall thickening of the thoracic aorta (arrows), causing occlusion of the right coronary ostium (arrowheads); (H) transesophageal echocardiography (TOE) showing circumferential thickening of the thoracic aorta; (I) TOE showing dilated right ventricle.
The patient tested positive for syphilis serology, with elevated titers of Treponema pallidum hemagglutination assay (TPHA) and venereal disease research laboratory (VDRL) testing. The remaining microbiological, serological and immunological tests were negative. A diagnosis of syphilitic aortitis with involvement of the RCA ostium was then made.
Surgical intervention was ruled out and, despite supportive measures, the patient died 72 hours after admission.
Dilatation of the AR and the AA, aortic thickness involving a coronary ostium and elevated VDRL and TPHA titers are highly suggestive of syphilitic aortitis. Syphilis is an etiology that, although rare, should be taken into account in the diagnostic approach of patients with acute myocardial infarction and coronary ostial stenosis.
Conflicts of interestThe authors have no conflicts of interest to declare.
