






A 44-year-old man with a diagnosis of non-ischemic dilated cardiomyopathy was referred for implantation of a cardiac resynchronization therapy (CRT) system with cardioverter-defibrillator (CRT-D) as primary prevention. The procedure was performed using the EnSite™ Precision™ (Abbott).
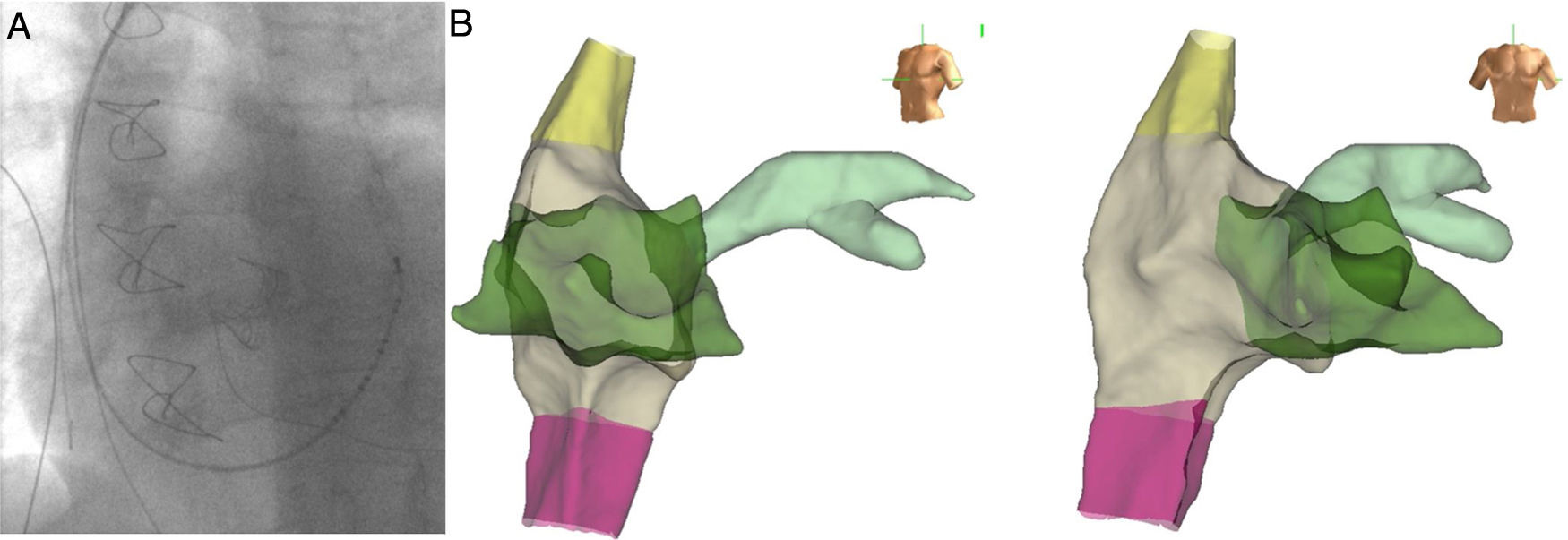
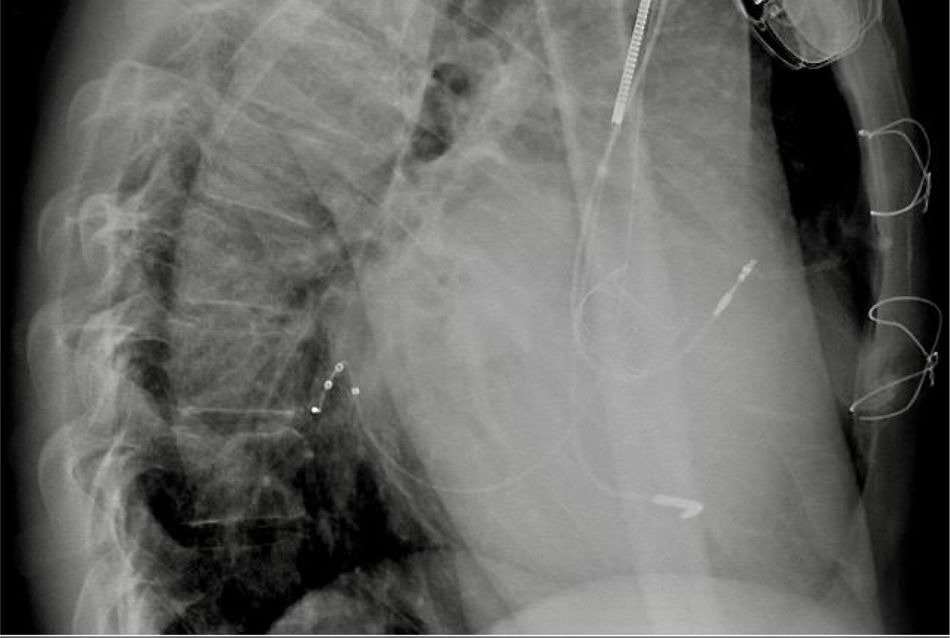
Via a subclavian vein approach, a 5F decapolar Response™ CSL electrophysiology catheter (Abbott) was used to create a three-dimensional (3D) model.1 After obtaining an endocardial shell the catheter was used to cannulate the coronary sinus (CS) (Figure 1). Under guidance by the electroanatomic system and very low dose fluoroscopy (to confirm that there was no catheter entanglement), a bipolar right ventricular (RV) lead was positioned in the RV apical septum. To continuously monitor the lead position (and identify possible lead dislodgment), the tip and ring poles were left connected to the EnSite system. The CS catheter was withdrawn and a sheath was used to catheterize the CS with the aid of the anatomic location on the 3D system. A guidewire (VisionWire; Biotronik) was inserted through the delivery system and connected to the EnSite system, and was used to map the anatomy and electrical activation of the CS branches (Figure 2). A branch was selected and the LV lead was placed in the latest site of ventricular activation (Figures 3 and 4). Using guidance by the navigation system and minimal fluoroscopy (hybrid approach), the right atrial lead was placed in a right appendage position, with real-time location of the other catheters (to check for possible displacement during manipulation of the atrial lead). Total procedure time was 96 min.
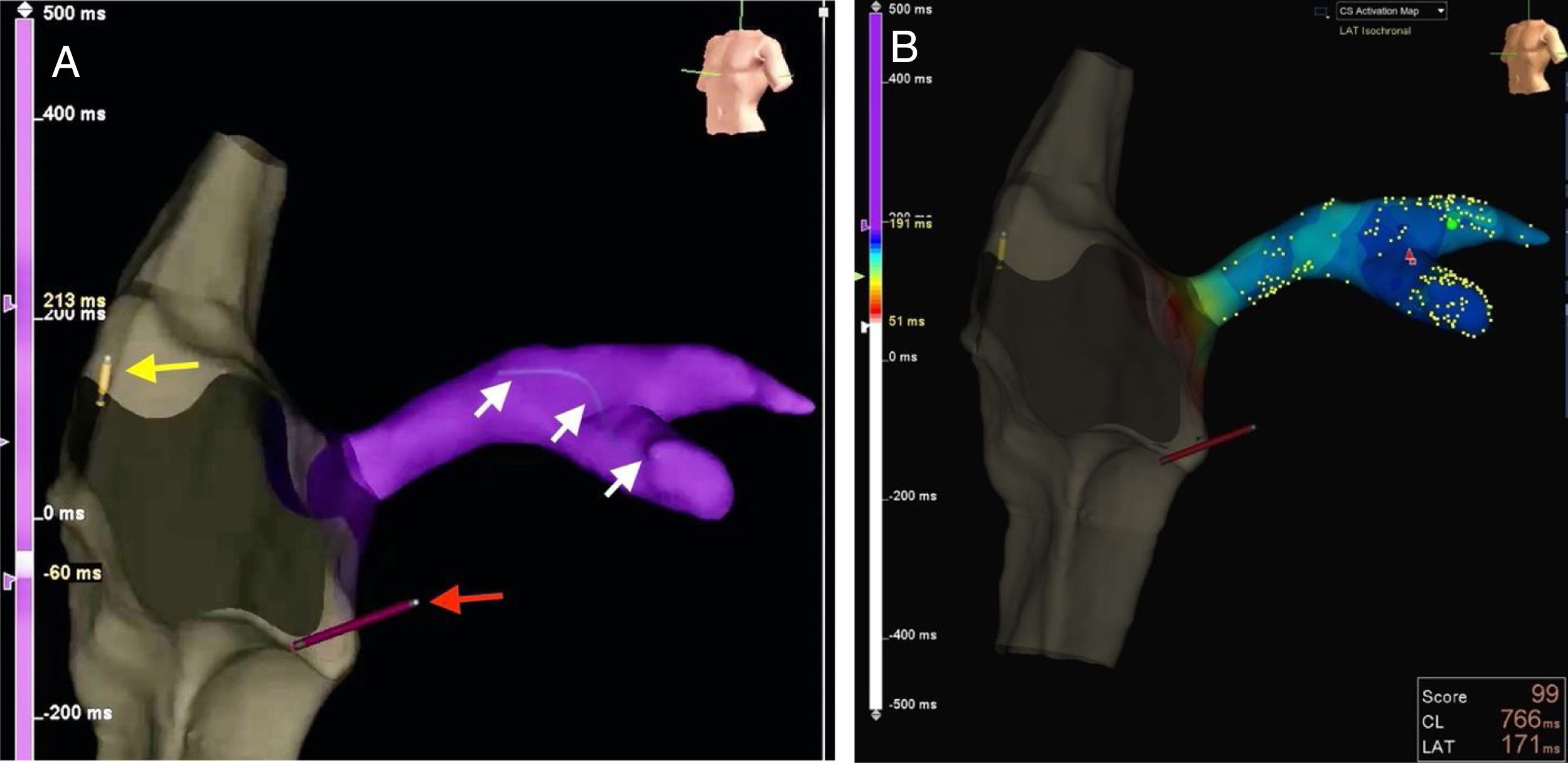
(A) Real-time visualization of catheter location (red arrow pointing to right ventricular lead, and yellow arrow to right atrial lead) and the VisionWire (Biotronik) inside the coronary sinus branches (white arrows); (B): electrical activation mapping of coronary sinus branches with guidewire and identification of the latest ventricular activation (mid segment of the lateral branch, dark blue).
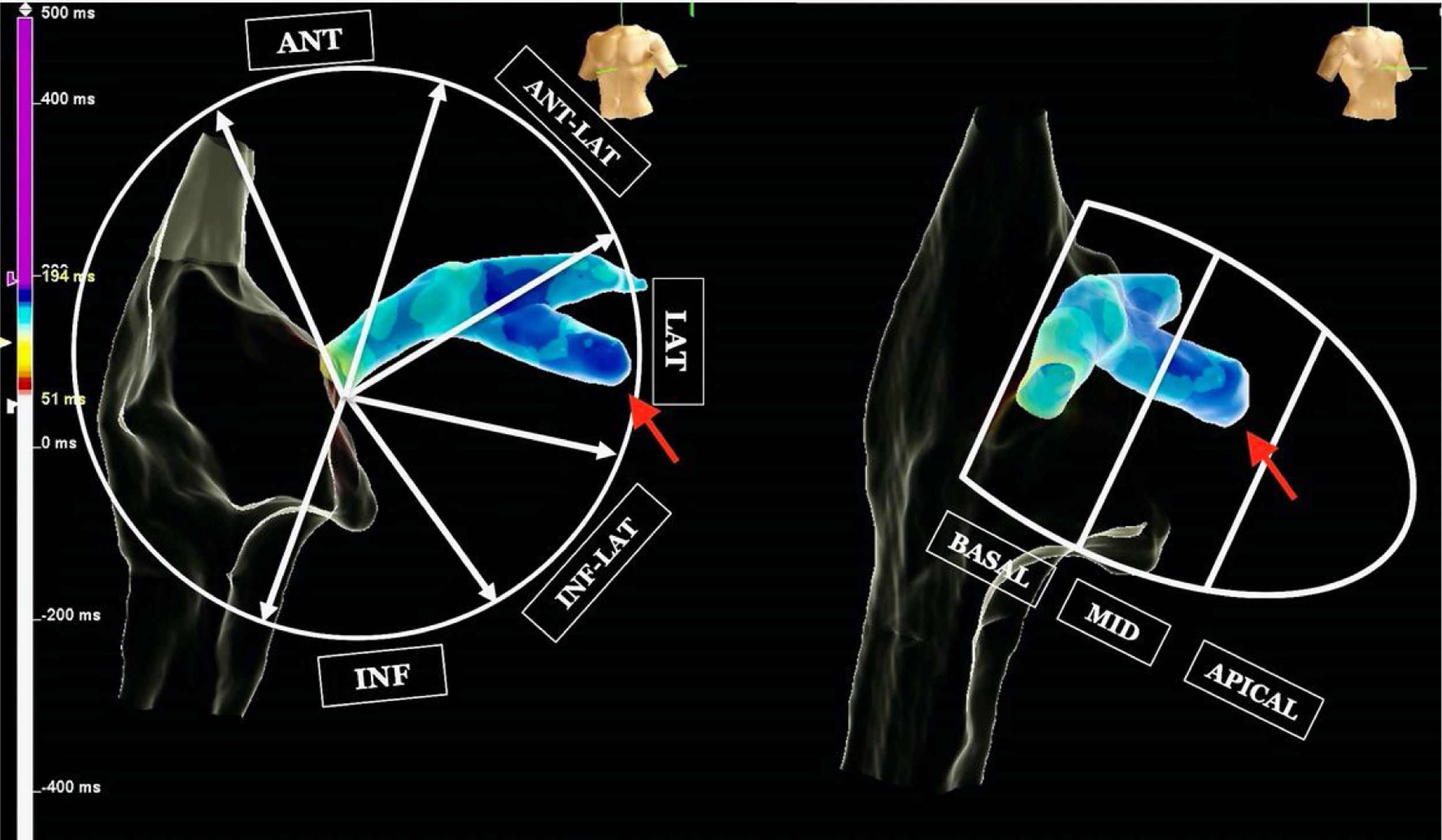
In this case the use of a 3D electroanatomic system with the VisionWire additionally enabled LV activation to be mapped, and guided optimal LV lead implantation toward segments of delayed LV activation (QRS width reduced from 165 ms to 100 ms with CRT on). This implantation approach allows a greater reduction in fluoroscopy and angiography times2–4 compared with the traditional technique of CRT implantation.
FundingThis work did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of interestThe authors have no conflicts of interest to declare.
