



A 34-year-old female with no cardiovascular history presented chest pain within two hours of a 38-week-gestation cesarean delivery. She was hemodynamically stable. Serum troponin I (2529.6 ng/l, cutoff 15.6 ng/l) and brain natriuretic peptide (508 pg/ml, cutoff 100 pg/ml) were elevated. Her electrocardiogram showed normal sinus rhythm (heart rate 50 bpm) without ischemic changes. Transthoracic echocardiography (TTE) revealed increased left ventricular (LV) dimensions, left ventricular ejection fraction (LVEF) 47%, global longitudinal strain (GLS) -19% with marked basal impairment, moderate central mitral regurgitation (MR) with apical displacement of the leaflet coaptation point, and normal right ventricular dimensions and function (Figure 1A, Table 1 and Video 1). Invasive coronary angiography revealed no lesions (Figure 2), while myocarditis was precluded by the absence of infection and pericardial effusion and normal serum C-reactive protein levels.

Transthoracic echocardiography. Bull's eye plot of left ventricular longitudinal strain showing (A) impaired values of basal walls in the acute phase and (B) their recovery one month later. ANT: anterior wall; ANT_SEPT: anteroseptal wall; INF: inferior wall; LAT: lateral wall; POST: posterior wall; SEPT: septal wall.
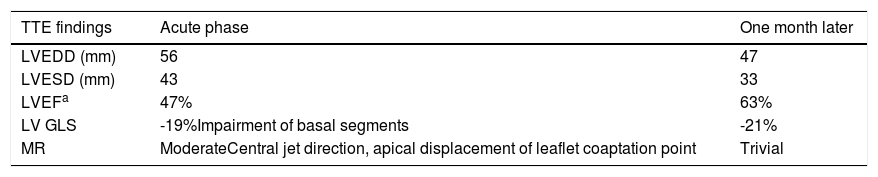
Transthoracic echocardiography findings indicating impaired basal left ventricular systolic function with basal ballooning in the acute phase and resolution of findings one month later.
| TTE findings | Acute phase | One month later |
|---|---|---|
| LVEDD (mm) | 56 | 47 |
| LVESD (mm) | 43 | 33 |
| LVEFa | 47% | 63% |
| LV GLS | -19%Impairment of basal segments | -21% |
| MR | ModerateCentral jet direction, apical displacement of leaflet coaptation point | Trivial |
GLS: global longitudinal strain; LV: left ventricular; LVEDD: left ventricular end-diastolic diameter; LVEF: left ventricular ejection fraction; LVESD: left ventricular end-systolic diameter; MR: mitral regurgitation; TTE: transthoracic echocardiography.
 Left anterior oblique view of the right coronary artery; (B) right anterior oblique view of the left coronary artery.")
One month later, repeat TTE revealed LV recovery (LVEF 63%, GLS -21% with apparent improvement in basal segments, trivial MR) (Figure 1B, Table 1 and Video 1). Meanwhile, cardiovascular magnetic resonance showed no late gadolinium enhancement and normal T2-weighted short tau inversion recovery imaging, while T1 and T2 mapping were consistent with low-grade edema at the basal septum where systolic dysfunction was noted in the acute setting (Figure 3). Indexed LV end-diastolic and end-systolic volumes were 110 ml/m2 and 33 ml/m2, respectively (LVEF 70%).
 Gadolinium study with no late enhancement; (B) T2-weighted short tau inversion recovery imaging showing no residual macroscopic myocardial inflammation or edema; (C) T1 mapping study and (D) T2 mapping study showing low-grade septal edema.")
Cardiovascular magnetic resonance one month after the acute phase. (A) Gadolinium study with no late enhancement; (B) T2-weighted short tau inversion recovery imaging showing no residual macroscopic myocardial inflammation or edema; (C) T1 mapping study and (D) T2 mapping study showing low-grade septal edema.
The physical and emotional stress associated with cesarean surgery, LV basal segment systolic impairment leading to basal ballooning and moderate functional MR (also enhanced by peripartum hemodynamic conditions) and the rapid recovery suggest basal Takotsubo cardiomyopathy.
Conflicts of interestThe authors have no conflicts of interest to declare.
