






The migration of African populations to Europe poses problems of adaptation that may increase the risk of cardiovascular disease. We assessed the cardiovascular risk of Cape Verdean university students studying in Portugal (CV-PT) compared to Cape Verdean university students in Cape Verde (CV-CV) and to Caucasian university students in Portugal (PT-PT).
MethodsA cross-sectional study was performed comparing three university populations, 54-62% female, aged 19-28 years: CV-PT (n=104), CV-CV (n=100) and PT-PT (n=100). Anthropometric data, blood pressure (BP), pulse wave velocity (PWV), albuminuria and estimated 24-h urinary sodium excretion (UNa+) using the Kawasaki formula were measured.
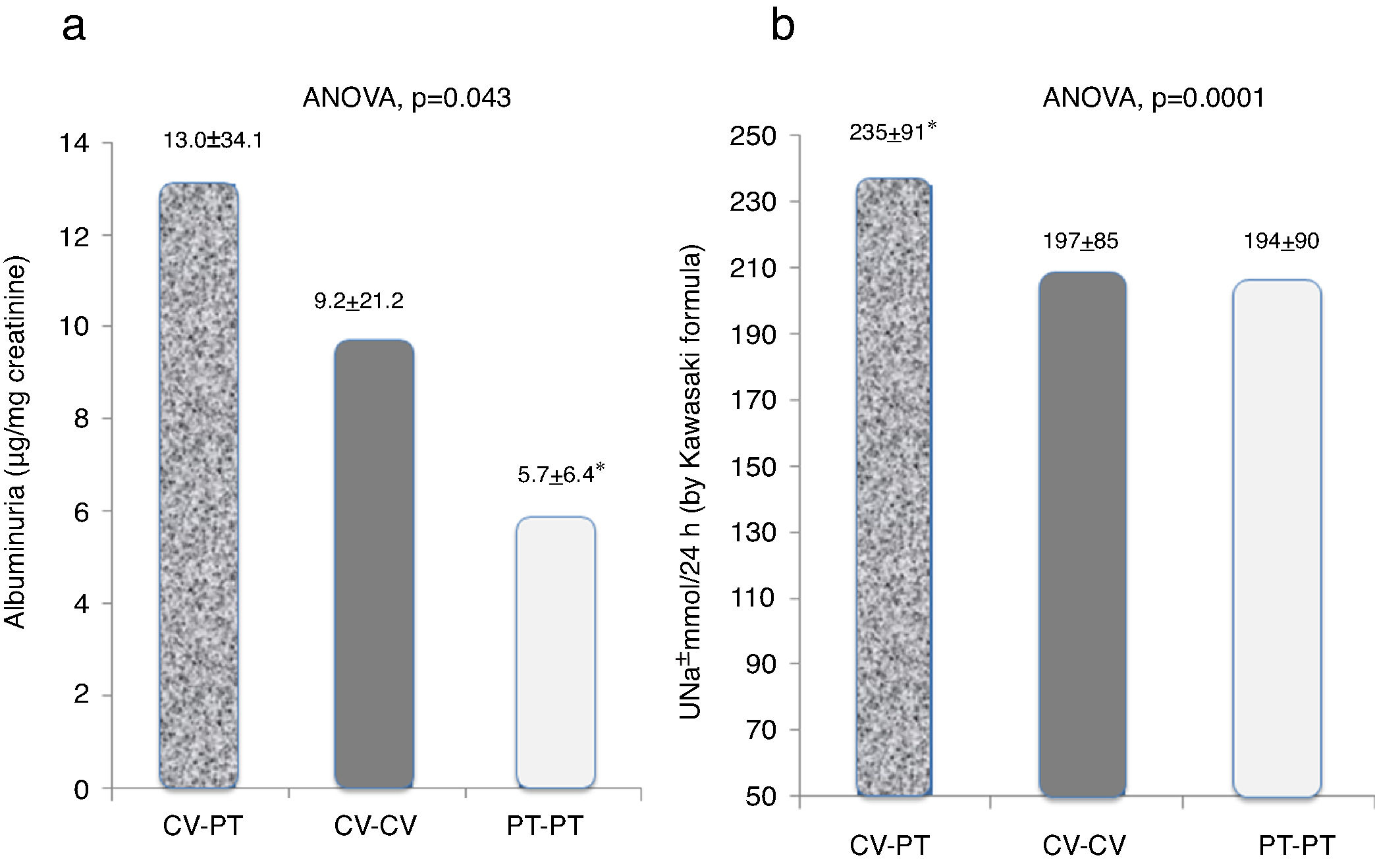
ResultsThe CV-PT group had higher body mass index and sodium intake (UNa+: CV-PT 235±91, CV-CV 197±85, PT-PT 194±90 mmol/24h; p<0.001), more sedentary lifestyles and worse socioeconomic, integration and adaptation indices compared to CV-CV and PT-PT. CV-PT and CV-CV also had higher systolic BP (CV-PT 119±12mmHg, CV-CV 121±15mmHg, PT-PT 107±14mmHg; p<0.001), PWV (CV-PT 8.7±1.1, CV-CV 8.8±1.8, PT-PT 8.0±1.2 m/s; p<0.04), and albuminuria (CV-PT 13.0±34.1, CV-CV 9.2±21.2, PT-PT 5.7±6.4μg/mg creatinine; p<0.04).
ConclusionCape Verdean university students in Portugal (CV-PT) have higher albuminuria, BP and PWV values than PT-PT and CV-CV students, associated with less healthy lifestyles, higher cardiovascular risk and worse socioeconomic conditions. The higher cardiovascular risk in these African immigrants means that it is important to implement measures to address modifiable risk factors, to improve integration and to promote healthy lifestyles.
O fenómeno de migração de populações africanas para a Europa coloca problemas de adaptação que podem propiciar um aumento do risco cardiovascular (CVas). É numerosa a população de estudantes de Cabo Verde (CV) a estudar em universidades portuguesas. Pretendemos avaliar níveis de adaptação socioeconómica e parâmetros de risco cardiovascular de estudantes de CV a estudar em Portugal (CV-PT) comparativamente a seus equivalentes a viver em CV (CV-CV) e a estudantes portugueses em Portugal (PT-PT).
MétodosEstudo transversal comparativo de três populações universitárias com 54-62% mulheres, entre 19-28 anos: CV-PT (n = 104), CV-CV (n = 100) e PT-PT (n = 100). Procedeu-se a avaliação clínica, da pressão arterial (PA, média de três registos), da velocidade da onda de pulso (PWV), da albuminuria (MA micg/mg creatinina) e da excreção urinária de sodium de 24h estimada pela fórmula de Kawasaki.
ResultadosA população CV-PT apresentou versus PT-PT e CV-CV piores índices socioeconómicos, de atividade física e de satisfação/integração e maior IMC, maior excreção urinária de sódio UNa+, CV-PT 235±91, CV-CV 197±85, PT-PT 194±90 mmol/24h (p = 0,001) e albuminuria, CV-PT 13,0±34,1, CV-CV 9,2±21,2, PT-PT 5,7±6,4 mcg/mg creatinina (p = 0,039). A população CV-PT apresentou versus PT-PT, PA sistólica mais elevada: CV-PT 119±12, CV-CV 121±15, PT-PT 107±14mmHg (p = 0,001) e maior rigidez aórtica, CV-PT 8,7±1,1, CV-CV 8,8±1,8, PT-PT 8,0±1,2 m/s (p = 0,038).
ConclusãoOs alunos cabo-verdianos a estudar em universidades portuguesas (CV-PT) apresentam alterações de marcadores de risco cardiovascular (PA, peso, rigidez aórtica e albuminuria) associados a estilos de vida, condições socioeconómicas e de integração piores do que os CV-CV e PT-PT. Esses achados impõem estratégias preventivas dirigidas à modificação das condições socioeconómicas e à promoção de estilos de vida saudável.
The increasing migration of populations of African descent to Europe poses problems of adaptation and health risk based on differences in genetic susceptibility and difficulty in adaptation to new socioeconomic, climatic and nutritional environments. This poses political, social and health challenges for host countries, exacerbated by the lack of accurate risk characterization of these migrant populations. The vulnerability of these populations is due to various factors, including novel socioeconomic, climatic and nutritional environments, and social differences such as linguistic and cultural barriers between the host countries and their countries of origin.1–7
The incidence and prevalence of cardiovascular disease vary considerably between ethnic groups. The determinants of these differences are not completely understood, but they are assumed to include variations in the presence and severity of different cardiovascular risk factors, differences in genetic susceptibility to each of these risk factors, and maladaptation to the new social and nutritional environments to which they are exposed.8
Cardiovascular disease is the leading cause of morbidity and mortality worldwide. Identification and treatment of modifiable risk factors can reduce the cardiovascular risk of individuals and populations. Morbidity and mortality associated with cardiovascular disease differ significantly between ethnic communities: populations of African origin have a significantly higher risk of cardiovascular events than Caucasian individuals, but it is unclear whether this difference results from greater genetic susceptibility or a phenotypic maladaptation to factors such as stress and different environmental conditions and lifestyles.1,9
The aim of this study was to assess the cardiovascular risk profile and lifestyles of Cape Verdean university students studying in Portugal and to compare them to those of Cape Verdean university students in Cape Verde and Portuguese Caucasian university students in Portugal, using non-invasive techniques.
MethodsA cross-sectional study was performed comparing three university student populations. The study protocol was approved by the ethics committee of Hospital S. João, Porto, and all participants gave their informed consent. The Order of Physicians and the National Committee for Ethics in Health Research of Cape Verde analyzed the protocol and in accordance to the legislation both institutions gave their tacit consent to the study, which was carried out according to the Declaration of Helsinki on the ethical principles for medical research involving human subjects. The number of Cape Verdeans studying at Portuguese universities is estimated to be over 5000. The study population was composed of Cape Verdean university students studying in Portugal for at least 12 months, Cape Verdean university students studying in Cape Verde, and Portuguese Caucasian university students studying in Portugal. The participants were all volunteers and were enrolled between January and April 2014. Recruitment and selection were based on official organizations and student associations in both Portugal and Cape Verde, which assisted in publicizing the study. Potential candidates were selected randomly from the databases of these organizations. All participants were examined on one visit, during which a complete assessment of each participant's anthropometric variables, personal and family history, social framework, diet and physical activity, physical examination, laboratory work-up (spot urine sampling) and office blood pressure measurements were performed. In addition, participants’ pulse wave velocity was measured using a validated non-invasive device.
MeasurementsAll measurements were performed by the same operator. Office BP was measured using an Omron 705IT automatic sphygmomanometer (Omron Healthcare, Hoofddorp, The Netherlands) with the patient in supine position after 10min of quiet rest, using appropriate cuffs for size of arms. The mean of three readings was recorded for the purpose of the present study.
Pulse wave velocity as a measure of arterial stiffness is an established cardiovascular marker, easy to assess, non-invasive and highly reproducible. Carotid-femoral pulse wave velocity, a well-characterized index of aortic stiffness, was calculated as previously reported10–12 using a validated non-invasive device (Complior; Colson, Garges lès Gonesses, France), which allows online pulse wave recording and automatic calculation of pulse wave velocity, obtaining two different pulse waves simultaneously at the level of the right common carotid and over the right femoral artery.
Albuminuria (μg/mg creatinine) and urinary sodium excretion were assessed in first morning spot urine samples. The Kawasaki formula13 was used to estimate 24-h urinary sodium excretion.14 Each subject's social framework and social adaptation were assessed through a confidential personal questionnaire applied during the visit. The validated questionnaire included questions regarding preferred and habitual method of transportation, monthly living expenses, type of accommodation, academic success (including semesters attended and semesters delayed), level of personal self-satisfaction regarding the new country and the university, and social integration. Diet and physical activity were also assessed through this questionnaire, including type, duration and frequency of physical activity, and consumption of drugs or alcoholic beverages and frequency.
Statistical analysisData are expressed as mean ± SD if normally distributed or as a percentage otherwise. Continuous variables in patient groups were compared by analysis of variance with the Bonferroni correction for multiple comparisons or by an independent Student's t test. Categorical variables were compared using the chi-square test. A two-tailed value of less than 0.05 was considered significant. All statistical analyses were carried out using SPSS software (version 15.0; SPSS Inc., Chicago, IL, USA).
ResultsA total of 304 university students, aged 19-28 years, male and female, were randomly selected to participate in the study. The study population constituted of 104 university students from Cape Verde studying in Portugal (CV-PT), 100 university students from Cape Verde studying in Cape Verde (CV-CV), and 100 Caucasian university students from Portugal studying in Portugal (PT-PT). Care was taken to ensure that the different study areas (medicine, technology, natural sciences or humanities) were similarly represented in the composition of the three groups. These three populations were compared in terms of anthropometric variables, personal and family history, social framework, diet and physical activity, physical examination, laboratory work-up (spot urine sampling), office BP and aortic stiffness.
The participants’ demographic characteristics, anthropometric measurements, personal and family history, physical activity and social framework are shown in Tables 1 and 2. The CV-PT population showed higher body mass index (BMI), less physical activity, more abuse of soft drugs, greater number of individuals with two or more cardiovascular risk factors, and more social maladaptation. Alcohol consumption was higher among the PT-PT and CV-CV populations than in the CV-PT population. The CV-CV and CV-PT populations included a larger number of individuals who had first-degree relatives with hypertension than the PT-PT population (Table 2). The CV-PT population more often shared accommodation and used public transportation (Table 2). As shown in Figure 1a, the CV-PT and CV-CV populations had significantly higher BP values than the PT-PT population. Both the CV-PT and CV-CV populations also presented significantly higher pulse wave velocity than the PT-PT population (Figure 1b). Both of the Cape Verdean student populations, whether living in Cape Verde or in Portugal, had significantly higher albuminuria values than their Caucasian counterparts (PT-PT) (Figure 2a). Albuminuria values were around 30% higher in the CV-PT population than in CV-CV, but this difference was not significant. As shown in Figure 2b, the population that had the greatest estimated urinary sodium excretion was CV-PT, significantly higher than in the PT-PT and CV-CV populations. Considering that each mmol of sodium excreted represents the excretion of around 5.8 mg of sodium chloride, the estimated mean salt intake was 13.6 g/day in CV-PT, 11.4 g/day in CV-CV and 11.2 g/day in PT-PT.
Demographic characteristics of the study population and medication taken.
| CV-PT | CV-CV | PT-PT | |
|---|---|---|---|
| n | 104 | 100 | 100 |
| Age | 22.5±2.6 | 24.9±3.3 | 23.5±3.0 |
| Female, % | 54 | 62 | 60 |
| BMI, kg/m2 | 22.9±3.5* | 21.9+3.8 | 21.6+3.1 |
| WC, cm | 79±9 | 78±12 | 78±9 |
| AHT medication, n | 1 | 0 | 1 |
| Other medication, n | 3 | 4 | 4 |
Personal and family history, physical activity and social framework.
| CV-PT | CV-CV | PT-PT | |
|---|---|---|---|
| n | 104 | 100 | 100 |
| >2 CV risk factors, n (%) | 14 (13.5)* | 4 (4) | 8 (8) |
| 1st degree relatives with hypertension, n (%) | 26 (25.0) | 33 (33) | 18 (18)* |
| Exercisea >3 times/week, n (%) | 7 (6.7)* | 29 (29) | 38 (38) |
| Alcohol >3 times/week, n (%) | 7 (6.7)* | 29 (29) | 38 (38) |
| Self-reported social maladaptation, n (%) | 40 (38.4)* | 25 (25) | 20 (20) |
| Abuse of soft drugs (>1 time/week), n (%) | 23 (22.1)* | 9 (9) | 12 (12) |
| Shared accommodation, n (%) | 100 (96.2)* | 29 (29) | 33 (33) |
| Public transport, n (%) | 62 (59.6)* | 30 (30) | 38 (38) |
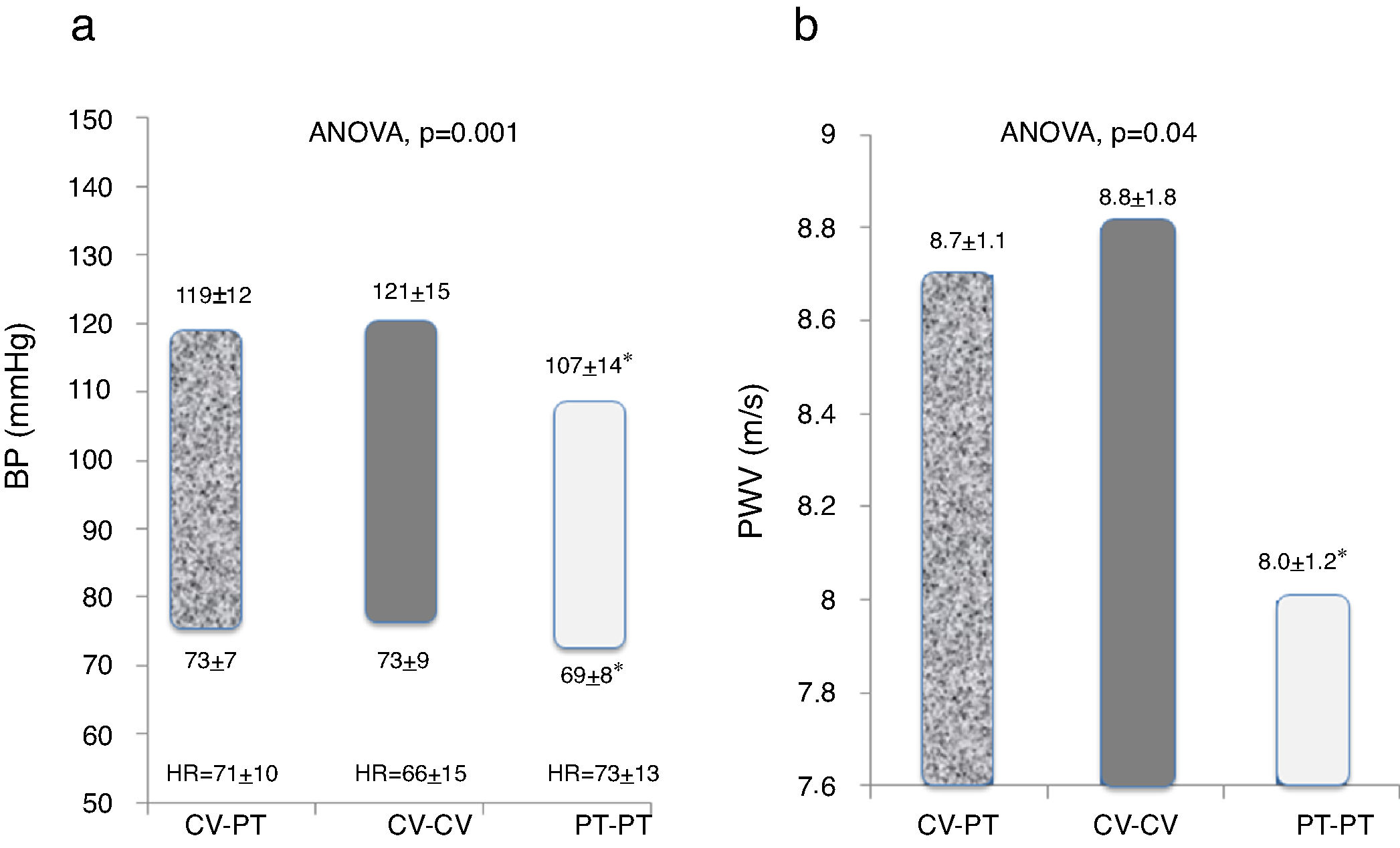
Blood pressure (a) and pulse wave velocity (b) in the study populations. ANOVA: analysis of variance; BP: blod pressure; CV-CV: Cape Verdean students in Cape Verde; CV-PT: Cape Verdean students in Portugal; HR: heart rate; PT-PT: Portuguese Caucasian students in Portugal; PWV: pulse wave velocity.
Cardiovascular disease is the leading cause of morbidity and mortality worldwide. Its incidence and prevalence vary between ethnic groups: it has been consistently reported that populations of black African origin, whether living in Africa, Europe or the US, have higher BP levels, greater frequency of hypertension, more cardiovascular risk factors, and greater associated morbidity and mortality.8,15–18
Movements and migrations of populations date back to before the beginning of recorded history.19 They pose social and health challenges for host countries, often exacerbated by the lack of accurate risk characterization of these migrant populations.8,19 The vulnerability of these populations is generally due to various biological, environmental, socioeconomic, psychological and medical factors.
To the best of our knowledge, this is a unique study, in which we compared the basic cardiovascular risk profile and social framework of university students of black African descent in Europe with those of European Caucasian university students in Europe and of black African university students living in Africa. Our study shows that the Cape Verdean university students who migrated to Portugal present various alterations that could be attributed to some degree of maladaptation to their new lifestyles and socioeconomic conditions. These include less physical exercise, more frequent drug abuse, more self-reported difficulties with social adaptation and integration, and indications of worse economic and social conditions compared to the other two groups. There were also significant differences in cardiovascular risk markers between these three young populations. Our study shows that even after a short stay as immigrants in Portugal, young Cape Verdeans living in Portugal already present important changes in cardiovascular risk profile, such as more sedentary lifestyle and higher BP levels, body weight, salt intake, aortic stiffness and albuminuria compared to similar individuals born and living in the host country (PT-PT), as well as higher salt intake, body weight and albuminuria compared to those born and living in their country of origin (CV-CV). This suggests that the increased cardiovascular risk associated with this population is closely associated with maladaptation and that specific early preventive measures may be justified. Obesity, salt intake and sedentary lifestyles are commonly associated,12 and it is plausible that persistence of these risk factors could increase the future risk of hypertension, increased aortic stiffness and cardiovascular complications. This is particularly important in young people with long life expectancy. Thus, one of the possible causes for the higher prevalence of cardiovascular risk markers in the CV-PT group is their poorer socioeconomic conditions due to maladaptation and related unhealthy lifestyles. In our study we found that these students have higher BMI and salt consumption than the other two groups. This suggests that dietary factors and lower levels of physical activity may also contribute to the differences found. Since the population sample were randomly selected, it appears that the observed lack of social adaptation and lower socioeconomic level are in fact the main discriminating feature of this population and that their greater cardiovascular risk may arise from these adverse conditions, as reported by others.20 Previous studies have shown high cardiovascular risk in immigrants in Europe21,22 and that compared with native Portuguese populations, African migrants have higher all-cause mortality and greater prevalence of circulatory disease, coronary heart disease and stroke.23 The higher education level of a population of university students compared to other sociocultural levels might be expected to act as a protective measure against the negative influences of change in environment. However, our study shows that significant alterations can already be identified in a group of young and highly educated students who on arrival are apparently healthy, and that even after a short stay as immigrants in Portugal these subjects already present important changes in cardiovascular risk profile, such as more sedentary lifestyle and higher BP levels, body weight, salt intake, aortic stiffness and albuminuria compared to similar individuals born and living in the host country, as well as higher salt intake, body weight and albuminuria compared to those born and living in their country of origin. These results suggest that this rapid development of cardiovascular abnormalities may be due to maladaptation to new socioenvironmental factors. Thus, our data indicate that particular attention should be paid to the prevention of cardiovascular disease in at-risk populations moving from their African countries of origin to European host countries.
The Portuguese university population (PT-PT) had a lower prevalence of hypertension than that observed in another study24 conducted 10 years ago of a sample nearly four times larger with similar BMI and age, although the proportion of hypertensive subjects is similar when the comparison is limited to the second academic year. Concern about the increase in cardiovascular risk among Portuguese adolescents has also been expressed.25
The limitations of the present study include those arising from the methodology of cross-sectional studies, especially when the population samples are relatively small. The lack of data on blood glucose levels, lipid profiles, liver and renal function and smoking may limit interpretation of the differences in cardiovascular risk between the groups.
ConclusionOur study shows that, comparing European Caucasian (Portuguese) and black African (Cape Verdean) university students, the latter, especially those studying in Portugal, have increased cardiovascular risk and indications of social maladaptation, presenting higher BP, arterial stiffness, albuminuria, and salt consumption values than their Caucasian counterparts. These results may help explain the higher cardiovascular risk and disease prevalence among blacks compared to non-blacks. The higher cardiovascular risk associated with these populations means that specific measures are justified to combat modifiable risk factors and to promote healthy lifestyles early in these individuals’ lives. Our study may contribute toward exploring and understanding racial differences in health and disease, particularly in cardiovascular health, risk and disease.
Conflicts of interestThe authors have no conflicts of interest to declare.
The authors would like to thank Dr. Emília Rosa da Silva Patrício (Hospital São João), Porto, for her assistance in the analysis of urine samples. They also would like to thank CINTESIS, Faculty of Medicine of the University of Porto, for making available their clinical exam room.
