



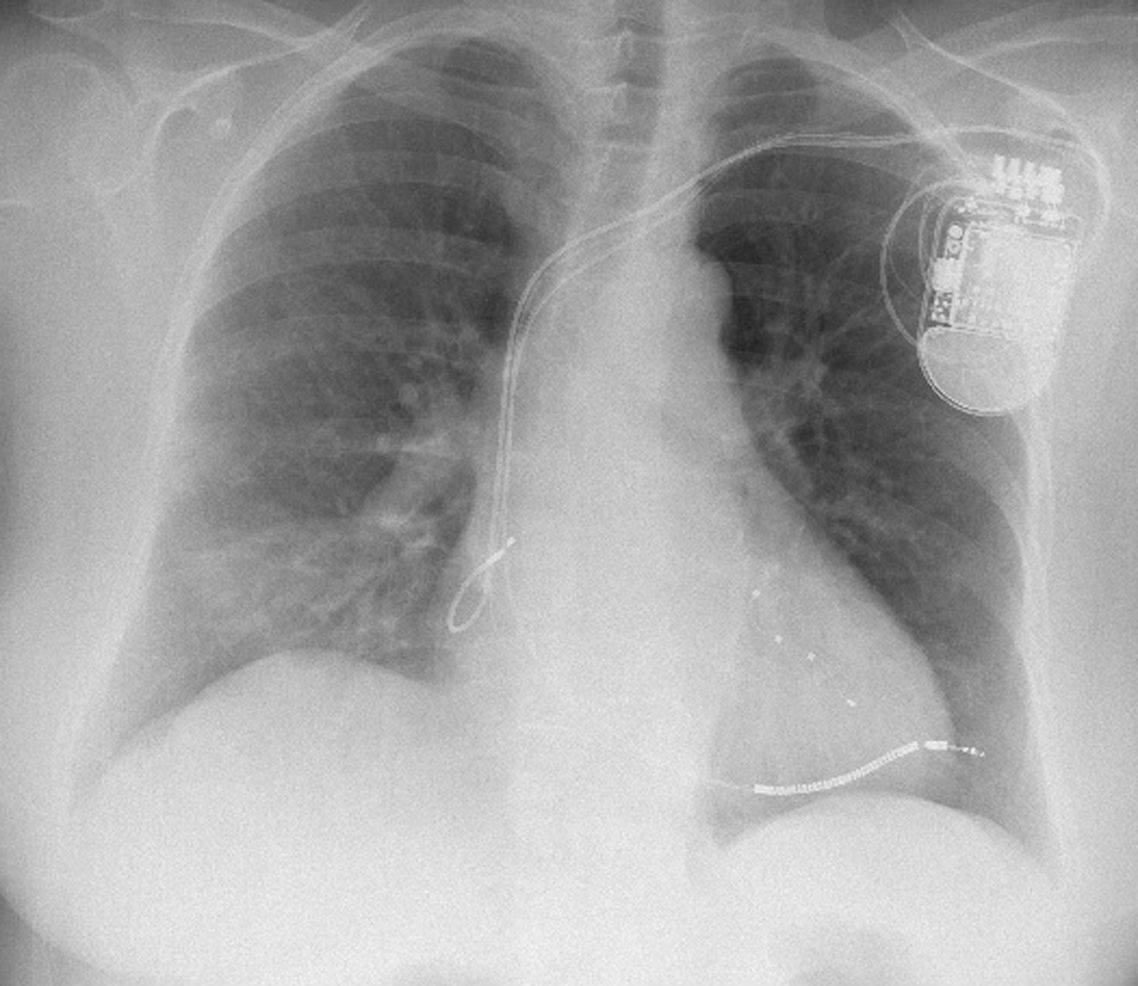
A 73-year-old woman with non-ischemic cardiomyopathy and left bundle branch block underwent implantation of a biventricular cardioverter-defibrillator with an active fixation, single-coil right ventricular lead. The procedure was without complications.
Three weeks later, she presented to the emergency department with complaints of pleuritic chest pain and shortness of breath. Her blood pressure was 100/40mmHg, oxygen saturation was 100% on room air and temperature was 38.2°C. Chest auscultation was normal and revealed no adventitious sounds. A chest radiograph demonstrated progression of the right ventricular lead beyond the cardiac silhouette (Figure 1), without hemothorax. Pericardial effusion was excluded. On interrogation of the device, reduced sensing amplitude was found.
Three sets of blood cultures were drawn before initiation of antimicrobial therapy with linezolid. Staphylococcus aureus was subsequently isolated.
We decided to extract the device since the patient had presented with fever and blood cultures were positive. Surgical backup was arranged and the pulse generator and leads were extracted by direct traction in the operating room with close echocardiographic monitoring. There was no pericardial effusion.
She remained stable and was discharged after a few weeks. Implantation of a new device was planned.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
