




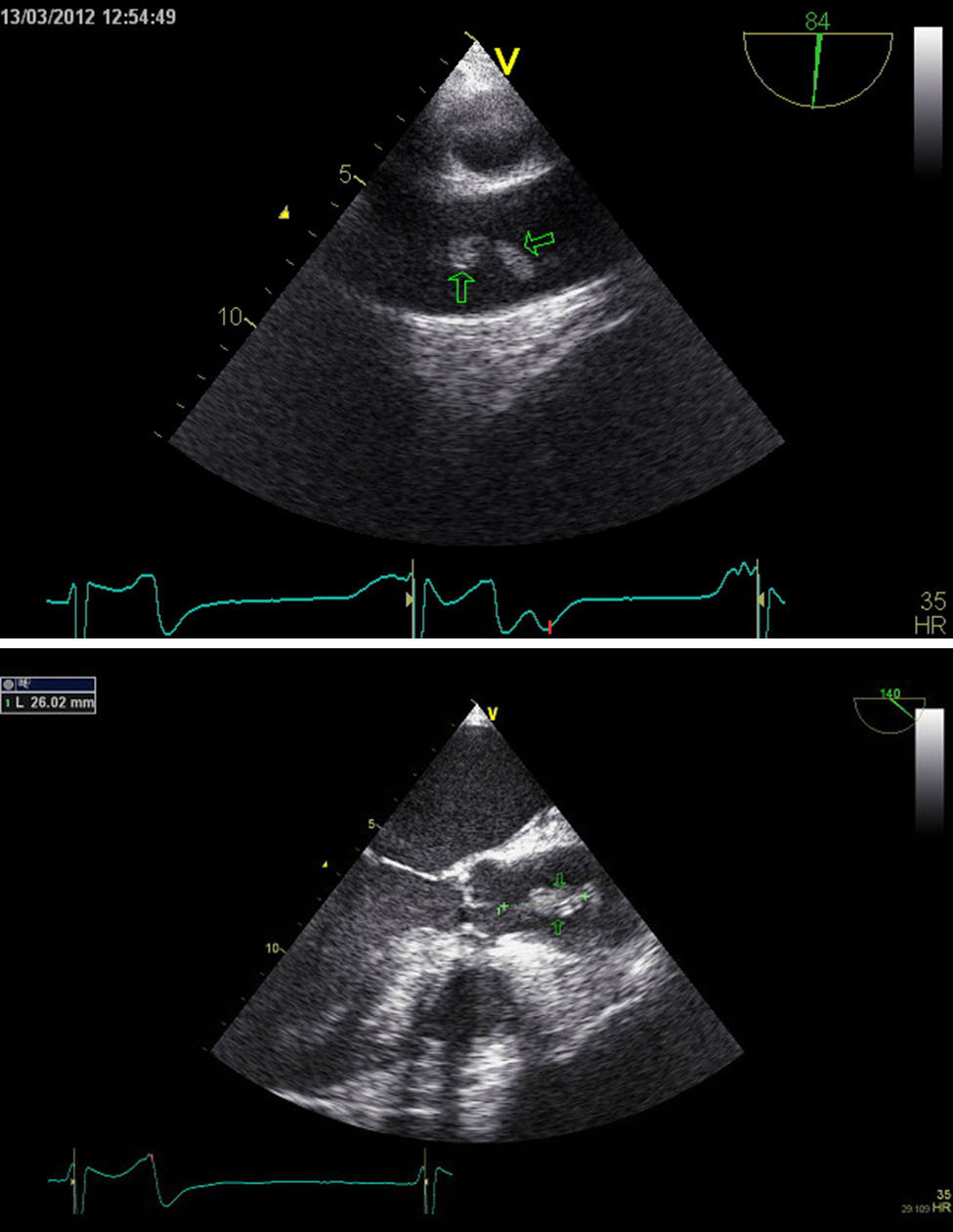
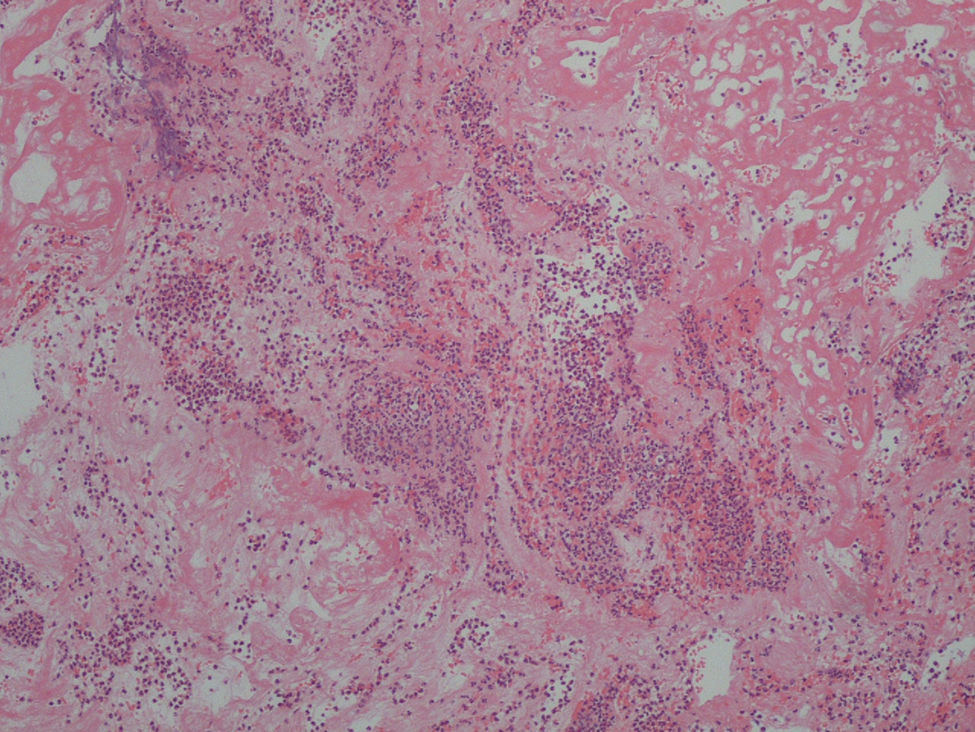
A 69-year-old man was admitted to the emergency room due to acute pulmonary edema. He had no known history of cardiovascular disease. The physical exam was notable for a harsh, grade IV/VI aortic systolic murmur and diffuse lung crackles. A transthoracic echocardiogram showed severe aortic stenosis, with normal biventricular systolic function. Coronary angiography was performed, as aortic valve surgery was envisioned. The next day the patient presented with fever and no other symptoms. Empirical antibiotic therapy was started. Blood cultures were drawn and methicillin-sensitive Staphylococcus aureus was identified, prompting a change in antibiotic therapy to vancomycin and gentamicin. Endocarditis was suspected and a transesophageal echocardiogram was performed. The exam showed a 14 mm pedunculated and highly mobile mass attached to the intima, protruding from the posterior wall of the ascending aorta, at the level of the sinotubular junction (Figures 1 and 2). Given the high embolic risk and to avoid the development of a mycotic aneurysm, the case was discussed with the cardiac surgeon and the patient was operated the next day. An inflamed ascending aorta was detected in the operating theater; the mass was excised and the ascending aorta and aortic valve were replaced. The histopathology was notable for aortic endarteritis, with granulocyte infiltration (Figure 3). After the operation, antibiotics were continued to complete an eight-week course. The patient was discharged thereafter. Our case illustrates a very rare location of a vegetation implanted in the aortic root, probably secondary to intimal trauma from prior coronary catheterization.
The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interestThe authors have no conflicts of interest to declare.
