




Secondary tumors are much more frequent than primary tumors, but cardiac metastasis of laryngeal carcinoma is uncommon.
The authors report the case of a 71-year-old man, with a history of laryngeal carcinoma, admitted to the emergency room with symptoms of two weeks’ evolution suggestive of respiratory infection. Due to lack of therapeutic response and progressive clinical deterioration, a transthoracic echocardiogram was performed which revealed a large infiltrating mass within the right ventricle, involving the apex, interventricular septum and free wall, not causing significant right ventricular outflow tract obstruction. Evaluation by computed tomography showed signs of widespread metastasis from the previously diagnosed laryngeal cancer.
Os tumores secundários são muito mais frequentes que os tumores primários; contudo, a metastização cardíaca do carcinoma laríngeo é incomum.
Apresentamos o caso de um homem de 71 anos, com antecedentes de carcinoma laríngeo, admitido no Serviço de Urgência por clínica sugestiva de infeção respiratória, com 2 semanas de evolução. Face à ausência de resposta terapêutica e deterioração clínica progressiva, realizou um ecocardiograma transtorácico, que revelou uma volumosa massa infiltrativa no ventrículo direito, envolvendo o ápex, septo interventricular e parede livre, não condicionando obstrução significativa do fluxo na câmara de saída. A avaliação imagiológica com tomografia axial computorizada mostrou sinais sugestivos de metastização difusa da neoplasia laríngea, previamente diagnosticada.
Secondary cardiac tumors have a higher incidence than primary tumors, occurring in 18% of patients with metastatic disease,1 but cardiac metastasis of laryngeal carcinoma is uncommon, with few cases reported in the literature.2,3
The authors report the case of a 71-year-old man with a history of laryngeal carcinoma, in whom a large infiltrating mass was detected in the right ventricle, compatible with a secondary lesion from laryngeal cancer.
Case reportA 71-year-old man, hypertensive and an ex-smoker, with a history of epidermoid carcinoma of the larynx diagnosed a year previously, had undergone total laryngectomy and lymph node drainage, together with adjuvant radiotherapy. He was admitted to our hospital with symptoms of two weeks’ evolution suggestive of respiratory infection. He also had atypical chest pain and worsening fatigue.
He had a history of treated pulmonary tuberculosis, chronic obstructive pulmonary disease, cerebrovascular disease and end-stage renal failure, but no previous history of cardiovascular disease.
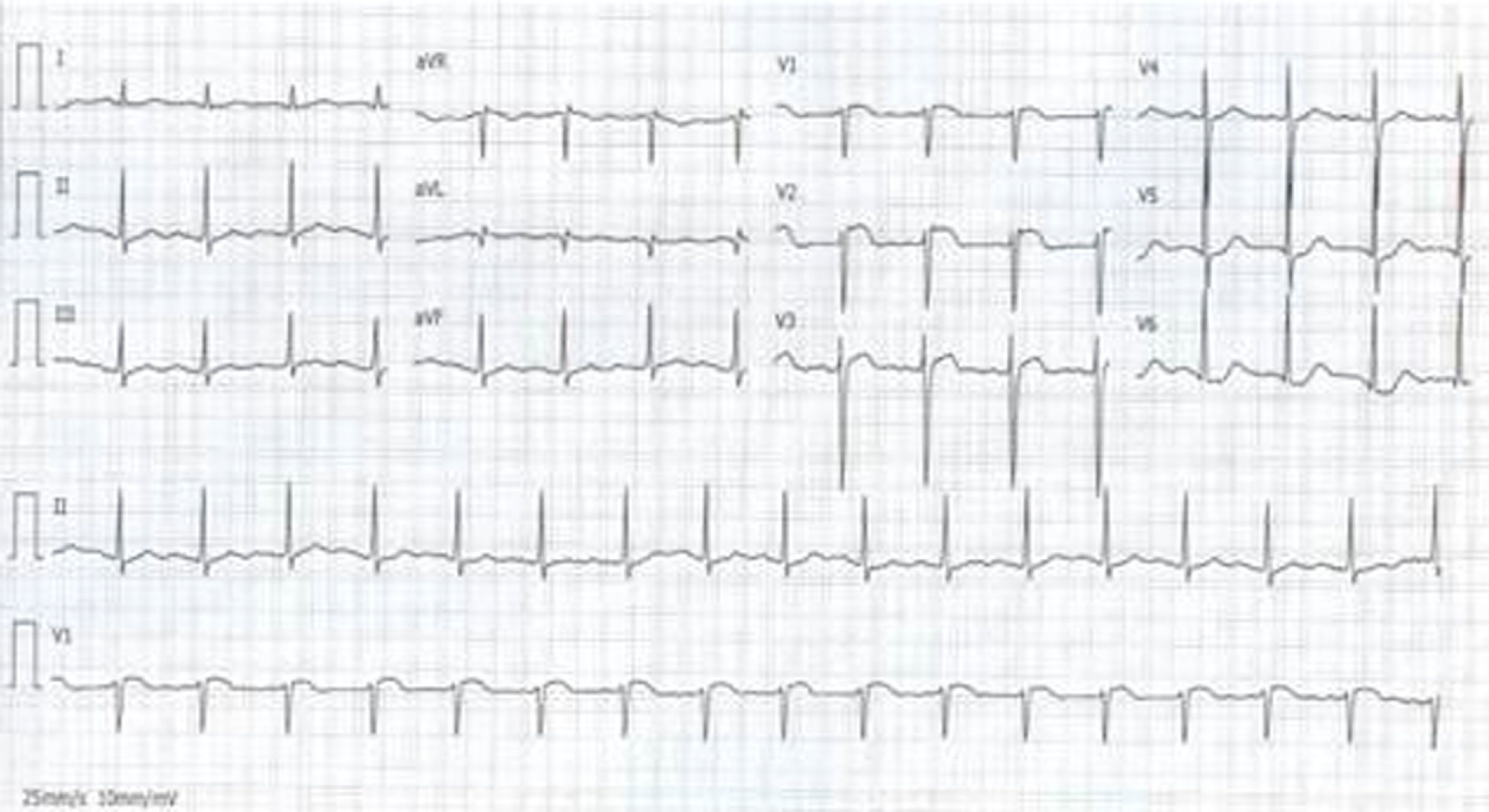
A chest X-ray in the emergency room revealed bilateral pulmonary infiltrate, with several nodular lesions and left pleural effusion. The electrocardiogram showed sinus tachycardia, poor R-wave progression and slight ST-segment elevation (<2mm) in leads V1–V3 (Figure 1). Laboratory tests showed no elevation of myocardial necrosis markers, but revealed anemia and significantly elevated inflammatory markers.
The patient was admitted with a diagnosis of community-acquired pneumonia. However, there was no therapeutic response to a series of different antibiotic regimens, and his general condition progressively deteriorated. Transthoracic echocardiography was accordingly performed (Siemens Acuson SC2000; 8V3c transducer), which showed a large infiltrating mass (45mm×40mm) in the apex of the right ventricle (RV), extending over the interventricular septum and the whole of the RV free wall up to the outflow tract (Figure 2). The mass was echogenic, with clearly defined edges and heterogeneous texture, but no sign of vascularization on color Doppler flow study. Despite slightly accelerated flow in the RV outflow tract, it did not cause significant obstruction (Figure 2D). Biventricular systolic function was preserved.
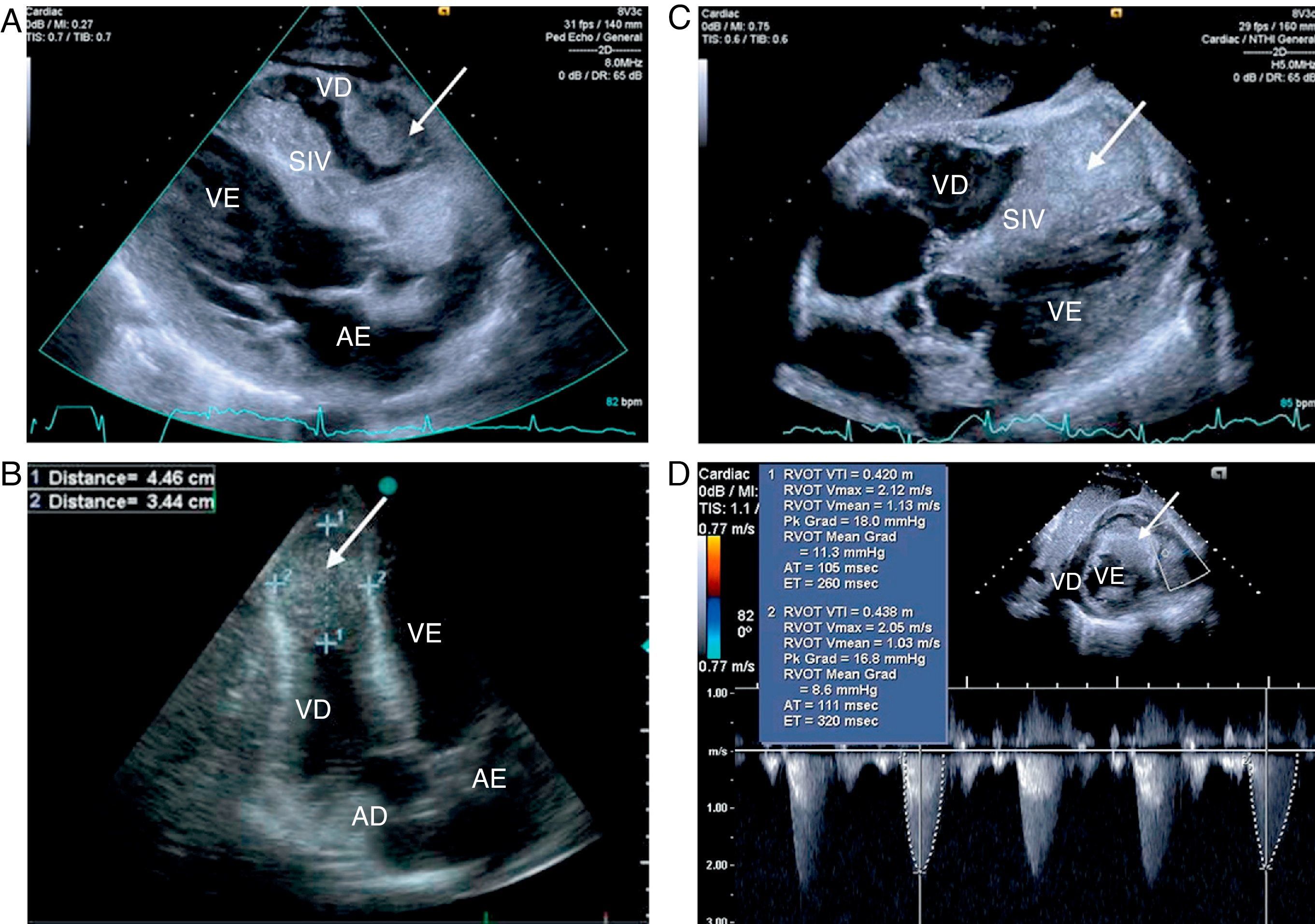
Transthoracic echocardiography (A–D), showing an infiltrating mass in the right ventricle (arrow), involving the entire apical region, interventricular septum and free wall, but not causing significant right ventricular outflow tract obstruction (D). AD: right atrium; AE: left atrium; SIV: interventricular septum; VD: right ventricle; VE: left ventricle.
In view of the patient's clinical history, the cardiac mass was interpreted as a metastatic lesion secondary to laryngeal carcinoma.
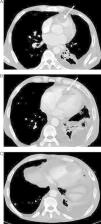
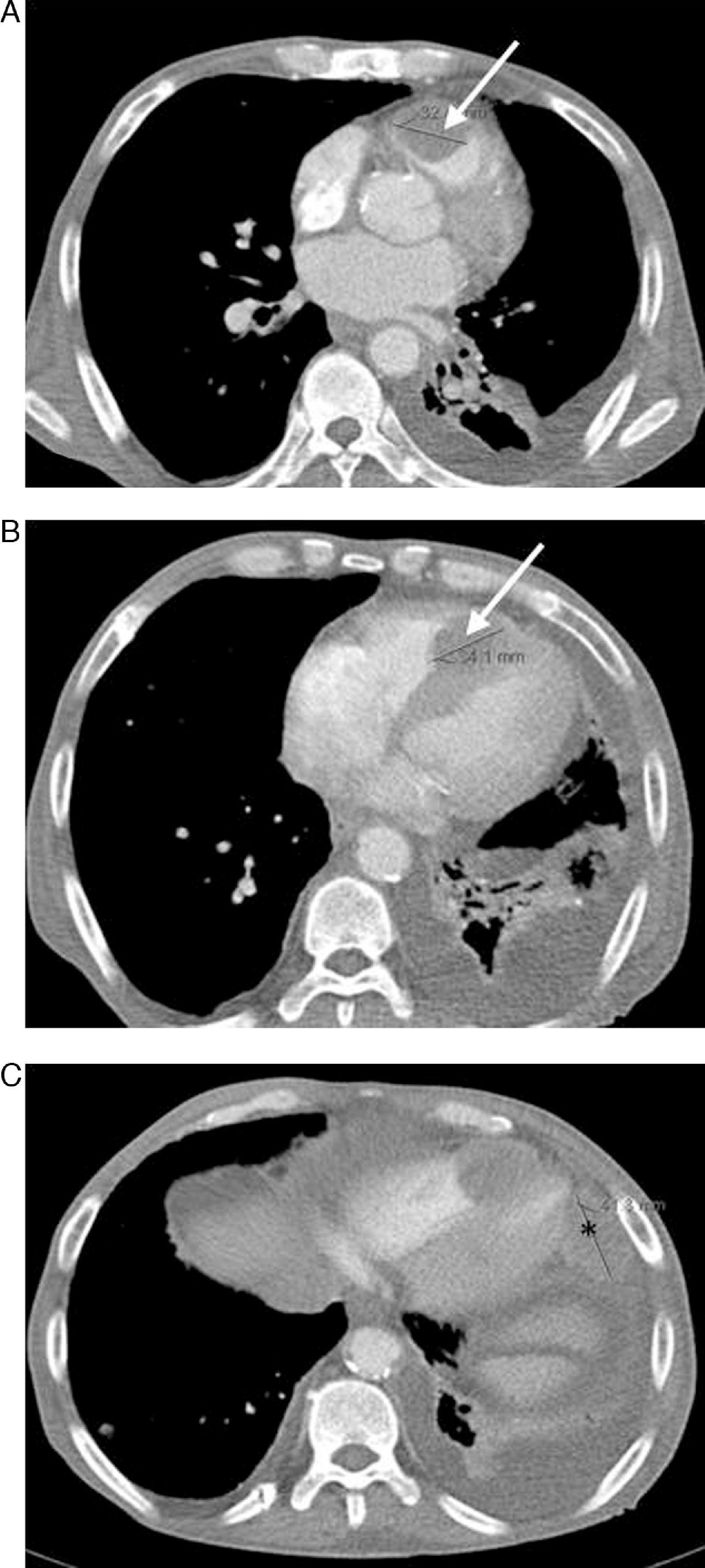
Cervical-thoracic-abdominal computed tomography (CT) was performed for disease characterization and staging, which showed signs of widespread metastasis involving the cervical region, lung, liver and adrenal tissue and bone, as well as confirming the presence of the RV mass (Figure 3A and B). Another mass was detected attached to the pericardium adjacent to the left ventricular lateral wall (Figure 3C).
In the light of these findings, a diagnosis of widespread metastasis from laryngeal cancer was established and palliative treatment was proposed.
DiscussionSecondary cardiac tumors are considerably more common than primary tumors but are one of the least investigated subjects in clinical oncology.4 A particularly high prevalence of cardiac metastases has been found in epidermoid lung carcinoma, urinary tract tumors and melanoma, although in absolute terms lung and breast tumors are more likely to metastasize to the heart.3,5
Metastasis can occur in various ways: through the lymph system, direct extension, and hematogenous or intracavitary dissemination by direct extension via the caval or pulmonary veins. Lymphatic propagation is the main mode of dissemination of cardiac metastases.1 Invasion of the mediastinal lymph nodes restricts lymphatic flow in the myocardium, promoting proliferation and migration of cancer cells to the epicardium. Around two-thirds of cardiac metastases involve the pericardium and a third the epicardium or the myocardium, while only 5% of tumors affect the endocardium.1 Generally, endocardial involvement results from hematogenous dissemination, while pericardial invasion mainly occurs through lymphatic propagation.1
Cardiac tumors are generally asymptomatic, most being detected following diagnostic investigation of an unrelated problem or in staging of a recently diagnosed primary tumor.1,3
The most common clinical manifestations are the result of large pericardial effusion, heart failure, obstruction of cardiac chambers or embolic phenomena.2,6,7 Cardiac tumors can also lead to rhythm disturbances, especially in atrioventricular conduction, as well as nonspecific changes on the electrocardiogram (ECG), particularly ST-segment and T-wave alterations. Although uncommon, invasion of the myocardium can cause sustained ST-segment elevation, mimicking acute transmural myocardial infarction.8
The case presented is of cardiac metastasis from laryngeal carcinoma, a rare entity that has seldom been reported in the literature. The clinical presentation, laboratory test results and the absence of evolving ECG changes were crucial for differential diagnosis.
More widespread use of high-quality diagnostic techniques has meant a greater number of such cases have been diagnosed in recent years. Echocardiography is the first-line imaging method to diagnose cardiac tumors,9 while CT and magnetic resonance imaging are valuable complementary exams, as they enable better characterization of the mass, as well as assessment of the involvement of extracardiac structures.10
Diagnosis of cardiac tumors is usually made in the advanced stages of the disease, which means that the various therapeutic options, including chemotherapy, radiotherapy and surgery, will only have limited success.
Patients with localized disease can be considered for neoadjuvant chemotherapy aimed at reducing the size of the mass sufficiently to proceed with complete resection. In such cases, it is important to perform a transvenous biopsy of the intracardiac mass guided by transesophageal echocardiography in order to determine the histological characteristics of the tumor and decide on appropriate therapy.7
In the rare cases in which metastasis affects the heart only and the primary tumor is controlled, treatment may even be curative with complete surgical resection of the mass.7 An alternative option for circumscribed secondary intracardiac tumors is embolization of the coronary branch supplying the mass.11
Palliative surgery also has a role in specific cases, such as obstruction of a cardiac chamber, cardiac tamponade, high risk of embolization or symptoms arising from local progression of the tumor.
Prognosis is highly dependent on the stage and histological aggressiveness of the tumor. Cardiac metastasis usually occurs in the context of disseminated carcinomatosis, which limits treatment to measures aimed at relief of symptoms.7 In the case presented, widespread metastasis from laryngeal cancer was presumed on the basis of imaging findings. Given the reliability of the imaging diagnosis and the patient's reserved prognosis, further invasive investigation, such as histological study, was considered unnecessary and inappropriate.
Management of these patients is complex, often requiring a multidisciplinary approach.
ConclusionsSecondary cardiac tumors are uncommon and generally detected in patients with widespread metastasis.
The case presented illustrates the inherent complexity of diagnosing cardiac tumors, largely due to the nonspecific nature of associated symptoms. It also highlights the importance of noninvasive imaging techniques for the diagnosis and prognostic assessment of cardiac metastases.
Conflicts of interestThe authors have no conflict of interest.
Please cite this article as: Rangel, I; Tumor metastático do ventrículo direito: um local incomum de envolvimento tumoral de carcinoma laríngeo. Rev Port Cardiol 2012. doi:10.1016/j.repc.2012.02.021.
