





The incidence of cardiac implantable electronic device infections has increased significantly over the years and they are associated with significant morbidity and mortality. The epidemiology in the Central region of Portugal is not known.
ObjectiveTo characterize cardiac implantable electronic device infections through a retrospective study of 3158 patients admitted to our center between January 2008 and September 2014 and to review the subject in the light of the current state of the art.
ResultsThe infection rate was 1.48% (pacemakers 1.21%, cardiac defibrillator/resynchronization devices 5.40%). The study population consisted of 47 patients with a mean age of 65±19 years, predominantly male (72.3%). Infections were mainly of pacemakers, the main device implanted in our population (n=2954), and most occurred late after first implantation. Clinically, most patients presented with fever and local inflammation. Blood cultures identified mainly Gram-positive microorganisms. Empiric antibiotic therapy with vancomycin was instituted in all patients, associated with gentamicin in 57%. The device was extracted in the majority of cases (72%). During follow-up (32±22 months) eight patients died (17%), seven of cardiovascular cause (15%), and seven were readmitted with device infection (15%).
ConclusionsOur rate of infection was low, similar to other published series, with a higher rate in cardiac defibrillator/resynchronization devices. After standard treatment with antibiotic therapy and device extraction, the prognosis was good.
O número de infeções associadas com dispositivos cardíacos tem aumentado exponencialmente ao longo dos anos. Estas infeções associam-se a elevada morbimortalidade. A sua epidemiologia na região centro do país não é conhecida.
Objetivo e métodosPretende-se caracterizar a nossa população de doentes com infeções de dispositivo através dum estudo retrospetivo, incluindo 3158 doentes consecutivos que implantaram dispositivos no nosso centro, entre janeiro de 2008 e setembro de 2014, e realizar uma revisão do tema à luz do estado da arte.
ResultadosA taxa de infeção na nossa população foi de 1,48% (pacemakers 1,21%, desfibrilhadores e dispositivos de ressincronização 5,40%). A população inicial era constituída por 47 doentes. Tinham idade média de 65±19 anos e predomínio do género masculino (72,3%). Foram predominantemente infeções em pacemakers, após primeira implantação e com surgimento tardio. A apresentação clínica foi variada, apresentando-se a maioria com febre e alterações inflamatórias locais. Identificaram-se nas hemoculturas, predominantemente, microrganismos gram positivos. A antibioterapia empírica inicial realizada foi vancomicina associada a gentamicina em 57% dos casos; extração do dispositivo foi realizada em 72%. Durante o seguimento (32±22 meses) morreram oito doentes (17%), sete dos quais de causa cardiovascular (15%) e verificaram-se sete reinternamentos por reinfeção (15%).
ConclusãoA taxa de infeção é baixa e semelhante a outras séries, sendo superior em desfibrilhadores e dispositivos de ressincronização. Após a admissão inicial para tratamento antibiótico±extração, o prognóstico foi bastante favorável.
Infections of non-valvular cardiac implantable electronic devices (CIED) – pacemakers and implantable cardioverter-defibrillator (ICD) or cardiac resynchronization therapy (CRT) devices – has increased in recent years,1–3 and now account for around 10% of cases of endocarditis.4 They are associated with significant morbidity and an 8.4-11.6% higher risk of mortality than with non-infectious cardiac device-related complications.5,6
Prevention or early diagnosis and treatment of CIED infection is crucial to survival and to reducing the risk of reinfection.7
There have been few studies on the subject and only recently has there been discussion of the best therapeutic approach. Current knowledge is based mainly on observational studies and there are as yet no international guidelines.
Epidemiological data on CIED infection in Portugal are almost non-existent, particularly for the Central region of the country. The aim of this study was to review the current state of the art, based on the experience of our center.
MethodsStudy populationWe performed a retrospective analysis of 3158 patients who underwent device implantation in our center between January 2008 and September 2014. Of these, 47 (1.48%) were hospitalized for CIED infection. The diagnosis was established according to the modified Duke criteria, based on the presence of localized pocket infection and/or endocarditis.
Baseline characteristicsThe following characteristics of the study population were recorded: age, gender, type of CIED, type of infection, type of implantation (replacement or first implantation), clinical presentation, known predictors of infection (hypertension, diabetes, oral anticoagulation, immunosuppression, smoking, long-term corticosteroid therapy, chronic renal disease, severe cardiac dysfunction, previous implantation of temporary pacemaker, antibiotic therapy prior to implantation and presence of hematoma following implantation.
Laboratory and imaging parametersLaboratory parameters at admission and during hospital stay were analyzed, together with the microorganisms isolated and the results of antibiotic susceptibility testing, and the findings of transthoracic (TTE) and transesophageal echocardiography (TEE) if performed.
Therapeutic approachThe initial empiric antibiotic therapy and any change following the results of susceptibility testing were recorded.
The method of device extraction (percutaneous or surgical), or the reason for not removing the device, and the timing of new device implantation were also analyzed.
Clinical follow-upPatients were followed for a mean of 32±22 months (10-54 months). The events considered during follow-up were rehospitalization due to device infection and mortality.
Statistical analysisThe statistical analysis was performed using SPSS® version 20. Continuous variables were expressed as means ± standard deviation and categorical variables as relative frequencies.
ResultsBaseline characteristicsThe mean age of the 47 patients admitted for CIED infection was 65±19 years, and 72.3% (n=34) were male.
Most of the devices involved were pacemakers (76.6%, n=36), followed by ICD (17%, n=8) and CRT devices (6.4%, n=3). The infection rate was significantly higher in patients with ICD or CRT devices (5.4%) compared to pacemakers (1.21%, p=0.04).
Sixteen patients (34%) had pocket infection, while the diagnosis was device-related endocarditis in the other 31 (66%).
Most infections (70.2%, n=33) occurred at least a year after implantation and were classified as late, and after first implantation (63.3%, n=30). There was a history of hospitalization for CIED infection in 38.3% (n=18).
Clinical presentation varied, but most patients (76.6%, n=36) presented with local inflammation manifested as redness, warmth and pain, with lead erosion in 42.6% (n=20). Fever occurred in 59.6% (n=28), and 25.5% (n=12) reported feeling general malaise, fatigue, weakness and loss of appetite. Three patients (6%) were admitted with fever of no apparent cause, diagnostic study revealing device-related infection.
Various known predictors of infection were identified in the study population: hypertension (61.7%, n=29), diabetes (44.7%, n=21), oral anticoagulation (17%, n=8), smoking (10.6%, n=5), long-term corticosteroid therapy (4.3%, n=2), chronic renal disease (8.5%, n=4) and severe cardiac dysfunction (21.3%, n=10). No patient had documented hematoma following CIED implantation or a temporary pacemaker prior to implantation of a permanent system. All had received prophylactic therapy with second-generation cephalosporin before device implantation (Table 1).
Characteristics of the study population.
| Infection rate, % | 1.44 |
| Pacemaker | 1.29 |
| ICD/CRT | 2.44 |
| Type of infection, % (n) | |
| Late-onset | 70.2 (33) |
| First implantation | 63.3 (30) |
| Previous infection | 38.3 (18) |
| Pocket infection | 72 (34) |
| Endocarditis | 28 (13) |
| Type of device, % (n) | |
| Pacemaker | 76.6 (36) |
| ICD | 17 (8) |
| CRT | 6.4 (3) |
| Clinical presentation, % (n) | |
| Signs of local inflammation | 76.6 (36) |
| Fever | 59.6 (28) |
| Erosion | 42.6 (20) |
| Systemic symptoms | 25.5 (12) |
| Fever of no apparent cause | 6.4 (3) |
| Embolic events | 4.3 (2) |
| Predictors of infection, % (n) | |
| Antibiotic prophylaxis prior to implantation | 100 (47) |
| Hypertension | 61.7 (29) |
| Diabetes | 44.7 (21) |
| Severe cardiac dysfunction | 21.3 (10) |
| Oral anticoagulation | 17 (8) |
| Smoking | 10.6 (5) |
| Chronic renal disease | 8.5 (4) |
| Long-term corticosteroid therapy | 4.3 (2) |
| Hematoma | 0 (0) |
| Temporary pacemaker | 0 (0) |
| Follow-up, % (n) | |
| In-hospital mortality | 8.5 (4) |
| Mortality during follow-up | 17 (8) |
| Reinfection | 14.9 (7) |
CRT: cardiac resynchronization therapy device; ICD: implantable cardioverter-defibrillator.
At least two blood samples were taken in all patients and microorganisms were isolated in 57.4% (27 patients), mainly Gram-positive bacteria: Staphylococcus aureus (eight), S. epidermidis (13) and S. hominis (two). Gram-negative microorganisms (Pseudomonas aeruginosa) were identified in four cases.
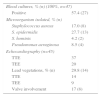
Echocardiography was performed in 45 patients, all except two with pocket infection. Thirty-seven underwent TTE, complemented by TEE in 12 cases. Vegetations were detected in 14 patients (29.8%), eight of whom had concomitant tricuspid valve involvement (Table 2).
Laboratory and echocardiographic findings.
| Blood cultures, % (n) (100%, n=47) | |
| Positive | 57.4 (27) |
| Microorganism isolated, % (n) | |
| Staphylococcus aureus | 17.0 (8) |
| S. epidermidis | 27.7 (13) |
| S. hominis | 4.2 (2) |
| Pseudomonas aeruginosa | 8.5 (4) |
| Echocardiography (n=45) | |
| TTE | 37 |
| TEE | 20 |
| Lead vegetations, % (n) | 29.8 (14) |
| TTE | 14 |
| TEE | 9 |
| Valve involvement | 17 (8) |
TEE: transesophageal electrocardiography; TTE: transthoracic echocardiography.
Empiric antibiotic therapy with vancomycin was instituted in all patients, associated with gentamicin in 27 patients (57%) who showed evidence of more severe infection. Based on the results of antibiotic susceptibility testing, therapy was adjusted to vancomycin alone in patients with secondary Gram-positive infection and to ciprofloxacin for those in whom Pseudomonas had been isolated.
The device was extracted in 72% of patients (n=34), the other 28% (n=13) being treated by medical therapy alone. Extraction was not performed in six patients with endocarditis and in seven with pocket infection. The decision to opt for medical therapy alone was prompted by evidence of localized pocket infection and/or the presence of comorbidities. The extraction procedure was surgical in 14 patients and percutaneous in the remaining cases.
A new device was implanted in 94% (n=32), performed within 48 h of extraction in all patients (Table 1); the other patients were not indicated for reimplantation.
Clinical follow-upFour patients (8.5%) died during hospitalization and eight (17%) during follow-up, of whom seven died of cardiovascular cause.
Albeit without statistical significance, there was a tendency for higher in-hospital mortality in patients with endocarditis and in those in whom the device was not removed. The same tendency was not seen with regard to in-hospital mortality.
There were seven rehospitalizations (14.9%) due to reinfection, mainly in patients with endocarditis.
No correlation was found between the type of microorganism and mortality or rehospitalization.
DiscussionBaseline characteristicsThere has been considerable growth in the number of devices implanted over the years, accompanied by a significant increase in cases of CIED infection.7,8 This is associated with high morbidity and mortality as well as significant costs9 and is due not only to the increase in the number of implants but also to more complex devices, a greater number of generator replacements and an aging target population with multiple comorbidities.7
The rate of CIED infection in our population was comparable to other studies, reported rates varying between 0.5-5%10 and 0.13-19.9% in pacemakers, and 0.0-3.2% in ICD/CRT devices,8,11–13 higher in more complex devices (dual chamber, larger generators or greater number of leads), which entail a more lengthy implantation procedure.
Infection may be confined to the pocket or may be systemic, with or without lead or valve endocarditis.14–16 Pocket infection can result from manipulation of the pocket during implantation or when the generator or leads erode through the skin; it can spread to downstream structures via the lead or through blood-borne dissemination from a remote site, or present as isolated bacteremia.6,11,17
Infections within a year of implantation (early) are probably due to contamination during the procedure, while those occurring after that period (late) are due to external contamination.10 However, the definition of early or late varies, with some centers considering late onset to be six weeks or three months after implantation.11 The time of onset from first implantation is important because it indicates not only the most likely etiological mechanism but also the ease of device extraction.11 Contamination of the pocket during implantation is more common with reintervention procedures and thus infections are more frequent following lead revision,8 which was not the case in our series.
The variability of presentation means a high index of suspicion is required. Most patients in our population had changes at the implantation site and fever. Besides signs of inflammation at the pocket site or erosion exposing the generator or leads, patients may also present nonspecific symptoms such as fatigue, loss of appetite, fever and chills or other systemic symptoms. Some cases are diagnosed on the basis of fever of no apparent cause in a patient with a CIED. Less common manifestations are pulmonary or systemic embolism, joint pain, spondylitis, pulmonary abscess or pleural effusion.11,2
Laboratory tests show changes related to systemic inflammation, including changes in white cell count, elevated C-reactive protein and higher erythrocyte sedimentation rate.2
Various risk factors for CIED infection are mentioned in the literature, many of which were seen in our population. These include diabetes, hypertension, chronic renal disease (particularly in patients under hemodialysis), long-term corticosteroid use, active malignancy, immunosuppression, oral anticoagulation, heart failure with left ventricular systolic dysfunction, reintervention (commonly due to hematoma, lead dislocation or device replacement), longer procedure times and more complex devices, implantation via abdominal access or thoracotomy, lack of antibiotic prophylaxis, fever in the 24 h before implantation and less experienced operators.18–21 Ideally, these risk factors should be controlled in order to reduce the risk of infection. Prophylactic antibiotics prior to implantation are particularly effective in this respect.22 Various observational studies have reported a greater than 50% reduction in CIED infection in patients receiving a single dose of antibiotics prior to the procedure.20,21 These findings are corroborated by a meta-analysis23 and by the results of a randomized trial in which the use of cefazolin reduced CIED infection from 3.28% to 0.64% (p=0.016) at eight months.24 There is no consensus on the best antibiotic or the duration of therapy; the choice will depend on whether methicillin-resistant Staphylococcus is present. There appears to be no benefit in continuing antibiotic therapy beyond the first dose or in applying antimicrobials or antiseptics to the pocket after implantation.25–28
Laboratory and imagining parametersAt least two blood cultures should be taken, ideally before antibiotic therapy is begun. The latest UK guidelines recommend that three blood cultures should be taken with ≥6 h between them, except in the presence of severe sepsis in which two blood cultures should be taken at different times within 1 h.28 Blood cultures should be taken again 48–72 h after removal of an infected CIED.28 Cultures are less often positive than in cases of valve endocarditis but they are reported in the literature to be positive in 80%–100% of patients with pacemaker-related endocarditis. At least two blood cultures were taken in all patients in our population and microorganisms were isolated in 57%. The low rate of positive results is probably related to samples being collected after antibiotic therapy, or may be due to slow-growing bacteria in a small number of cases. Besides usual culture in aerobic and anaerobic media, cultures should be performed for fastidious microorganisms, fungi and mycobacteria,29 which was not done in our center.
In cases of erosion, pocket-site tissue should be sent for culture, but percutaneous aspiration of the device pocket should not be performed as part of the diagnostic evaluation and is considered contraindicated if there is no erosion.13
Culture of the removed leads offers the possibility of an etiological diagnosis in the majority of cases and is therefore mandatory. Sterile manipulation after removal and rapid submission to the laboratory are essential.
As found in our population, most infections are monomicrobial,13,30 involving coagulase-negative staphylococci, mainly S. epidermidis and S. aureus. Only 10-30% are due to other Gram-positive microorganisms like Enterococcus, Streptococcus, and Corynebacterium spp. and Propionibacterium acnes, Gram-negative bacteria such as Enterobacteriaceae and Pseudomonas, atypical bacteria like Nocardia spp., fungi like Candida and Aspergillus and mycobacterial organisms.12,31 The increasing incidence of multiresistant microorganisms indicates that many infections are acquired in the hospital environment.
Infections by S. aureus are more serious and are associated with higher mortality32 compared to other microorganisms (9% vs. 4%).31
The chest X-ray can detect associated lung infection, pulmonary abscess and pleural effusion.
Echocardiography plays a central role in the diagnosis of CIED infection33 as it can detect and assess vegetations, which may be located on leads, the tricuspid or other valves or the endocardium. Vegetations do not always appear as masses attached to structures but may present as a filiform structure or as localized thickening of the lead, making diagnosis more difficult.
TTE has low sensitivity and negative predictive value for detecting vegetations on cardiac devices, while TEE has higher specificity and sensitivity.11 The two modalities are complementary and should both be used as part of an overall assessment.33
The presence of lead-induced echoes, atypical location of vegetations and inadequate acoustic window may produce false negative results, and so the lack of visible vegetations does not rule out CIED infection; when clinical suspicion is high, repeat TEE is warranted within seven days.33
Echocardiographic study should also be performed after device extraction to exclude residual vegetations, particularly of the right ventricle, tricuspid valve, right atrium and superior vena cava.29
Echocardiographic images should be carefully interpreted in the light of the available clinical information. An incidental finding of small masses adhering to leads should be considered in the diagnosis but these may be fibrous tissue or thrombi rather than vegetations.13
Two patients in our population with pocket infection did not undergo echocardiographic study, possibly because in the earlier years of the study period there were no protocols establishing all the diagnostic exams to be performed.
Other imaging modalities can be used to aid diagnosis, such as 99mTc-labeled leukocyte scintigraphy, which can show uptake of the marker in areas of infection in doubtful cases. 18F-fluorodesoxyglucose positron emission tomography has also been found useful in the diagnosis of CIED infection, but experience is limited and further validation of this method is needed.34,35
Suspected pulmonary embolism should be confirmed by thoracic computed tomography angiography or ventilation-perfusion scintigraphy.
Since the Duke criteria were found to be insufficiently sensitive, the modified Duke criteria have been established in order to standardize diagnosis, and now include local signs of infection and pulmonary embolism as major criteria29 (Table 3).
Modified Duke criteria.
| 1. Definitive infective endocarditis |
| Pathological criteria |
| Microorganisms demonstrated by culture or histologic examination of a vegetation, a vegetation that has embolized, or an intracardiac abscess specimen; or |
| Microorganisms demonstrated by culture of the lead tip |
| Clinical criteria: 2 major or 1 major and 3 minor or 5 minor |
| Major |
| Blood culture positive for infective endocarditis |
| Typical microorganisms from two separate blood cultures, defined as follows |
| Microorganisms consistent with endocarditis in two blood cultures drawn ≥12 h apart, or |
| All of three blood cultures or a majority of four separate cultures, with first and last sample drawn at least 1 h apart |
| Evidence of endocardial involvement |
| Vegetations on echocardiogram |
| Intracardiac mobile masses on leads or on the endocardium in contact with leads |
| Abscess in contact with leads |
| Minor |
| Fever (>38°C) |
| Vascular phenomena |
| Immunologic phenomena |
| Echocardiographic images suggestive of endocarditis |
| Positive blood cultures that do not meet major criteria |
| 2. Possible infective endocarditis |
| 1 major criterion and 1 minor criterion; or 3 minor criteria |
| 3. Diagnosis of endocarditis rejected |
| Firm alternate diagnosis; or |
| Resolution of infective endocarditis syndrome with antibiotic therapy for ≤4 days; or |
| No pathologic evidence of infective endocarditis at surgery or autopsy, with antibiotic therapy for ≤4 days. |
Before the establishment of the modified Duke criteria, others were proposed such as the modified von Reyn criteria or those established by Chamis11 (Table 4).
von Reyn criteria.
| 1. Definitive diagnosis |
| Isolation of microorganism on histologic or bacteriologic testing of vegetation or peripheral embolus |
| 2. Probable diagnosis |
| ≥2 positive blood cultures plus one of the following: |
| New regurgitant murmur |
| Previous heart disease (congenital or acquired) |
| ≤2 positive blood cultures plus fever plus new regurgitant murmur plus vascular phenomena |
| 3. Possible diagnosis |
| ≥2 positive blood cultures plus one of the following: |
| Vascular phenomena |
| Previous heart disease (congenital or acquired) |
| ≤2 positive blood cultures plus fever plus previous heart disease plus vascular phenomena |
| For viridans streptococcal cases: ≥2 positive blood cultures without an extracardiac source |
| 4. Diagnosis rejected |
| Alternate diagnosis generally apparent |
| Culture-negative endocarditis |
Antibiotic therapy should be initiated early. In the light of current knowledge of the causal agents involved, antibiotic coverage for Gram-positive methicillin-resistant bacterial strains is recommended, vancomycin being the most commonly used drug. This should be combined with coverage for Gram-negative bacteria in patients with sepsis. Therapy should be adjusted appropriately following confirmation of the microorganism involved.13
The duration of antibiotic therapy varies after device extraction, ranging from two weeks in cases of pocket infection to 4-6 weeks in cases of confirmed endocarditis, especially if blood cultures remain positive.13
Treatment with antibiotic therapy alone, without device extraction, is associated with frequent reinfection and higher mortality.36 Various studies have shown that there is a particularly high risk in S. aureus bacteremia, even in the absence of visible CIED infection, and so device removal is recommended.12,32 In cases of Gram-negative bacteremia, the risk of device infection appears to be low, and thus extraction is not mandatory unless there is reinfection after appropriate antibiotic therapy.12,36
Together with antibiotic therapy, complete device removal is essential, irrespective of the extent of infection. The only exception in some guidelines is antibiotic therapy alone with an agent with activity against staphylococci for 8-10 days for superficial or incisional infection, if there is no involvement of the device.12 Conservative treatment is often ineffective and is associated with high mortality (31-66%, as opposed to 13-21% with combined treatment).6,37 Device removal should be performed early rather than after a period of antibiotic therapy.
In our population we opted not to remove the device in some patients with localized pocket infection only and in others with multiple comorbidities at high risk during the extraction procedure. To date there have been no rehospitalizations for reinfection in these cases; however, there was a tendency for higher in-hospital mortality in patients who did not undergo device removal.
The extraction procedure is more difficult in the case of late-onset infections, and carries a higher risk of complications due to the formation of fibrocollagenous tissue.11
Reimplantation of a new deviceReimplantation should not be an automatic decision and the original indication for the device should be reassessed. According to the literature replacement is not indicated in around one third of patients with a diagnosis of CIED infection.13 When reimplantation is needed, it should be performed on the contralateral side or by epicardial implantation. There are no randomized trials to guide the timing of reimplantation; this depends on the type of infection, the presence of positive blood cultures, and the pathogen involved. Patients with no evidence of endocarditis and positive blood cultures can be reimplanted if repeat blood cultures after CIED removal remain negative for 72 h. In the event of valve infection, reimplantation should not be performed until at least 14 days after the first negative blood cultures after CIED removal.13 Patients who are pacemaker dependent are a real challenge in terms of the extraction approach. Implantation of a temporary pacing system enables completion of antibiotic therapy, thus reducing the risk of infection of the new device, but the rate of complications such as dislocation or infection of the temporary lead and right ventricular perforation is significant.38 An alternative is to implant a new conventional system at the same time or an epicardial system. A new and increasingly popular approach that provides a bridge of 10-15 days of antibiotic therapy prior to implantation of a new device consists of implantation of an active-fixation right-ventricular lead via the jugular vein that is sutured to the skin and connected to a VVI generator placed in an antimicrobial envelope and covered with an adhesive dressing.39
Clinical follow-upMortality in our series was similar to that reported in the literature: 4-10% in-hospital and 15-20% at one year.13 It is higher at one year in cases of healthcare-associated infection, multiresistant staphylococcal infection,6 concomitant valve involvement and medical therapy alone.2
Areas of uncertaintyAs stated above, randomized trials are needed to determine the best approach to various issues, including the duration of antibiotic therapy, the timing of device reimplantation, and the type and duration of antibiotic prophylaxis.
Further studies are also required on patients with positive blood cultures but no other evidence of endocarditis, in order to standardize treatment.
The role of leadless pacemakers and subcutaneous ICDs should also be investigated as results indicate a lower rate of infection with these devices.
LimitationsThe study has the following limitations: this was a single-center series with a short follow-up; collection of material during the extraction procedure was not systematic; TTE was not performed in all patients; and the device was not removed in all patients with indication for extraction.
ConclusionCIED infection is a serious, potentially life-threatening complication. Although guidelines exist, the approach to these patients has yet to be standardized, even in centers treating a large volume of cases; this is particularly true of prophylactic therapy prior to implantation, and treatment of infection when diagnosed.23 Protocols covering the diagnosis and treatment of CIED infection are required.
The rate of infections in our center was similar to that reported in the literature, and most were late-onset infection of pacemakers. Clinical presentation varied, but in most cases Gram-positive microorganisms were isolated. There were no CIED infection-related rehospitalizations or deaths during follow-up.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Fernandes A, Cassandra M, Trigo J, et al. Endocardite de dispositivos, revisão com base na experiência de um centro. Rev Port Cardiol. 2016;35:351–358.
