


Atherosclerotic cardiovascular disease (ASCVD) remains the major cause of premature death and disability; effective cardiovascular (CV) risk prevention is fundamental. The World Heart Federation (WHF) Cholesterol Roadmap provides a framework for national policy development and aims to achieve ASCVD prevention.
At the invitation of the WHF, a group of experts from the Portuguese Society of Cardiology (SPC), addressed the cholesterol burden at nationally and discussed possible strategies to include in a Portuguese cholesterol roadmap. The literature review showed that the cholesterol burden in Portugal is high and especially uncontrolled in those with the highest CV risk. An infographic scorecard was built to include in the WHF collection, for a clear idea about CV risk and cholesterol burden in Portugal, which would also be useful for health policy advocacy.
The expert discussion and preventive strategies proposal followed the five pillars of the WHF document: awareness improvement; population-based approaches for CV risk and cholesterol; risk assessment/population screening; system-level approaches; surveillance of cholesterol and ASCVD outcomes. These strategies were debated by all the expert participants, with the goal of creating a national cholesterol roadmap to be used for advocacy and as a guide for CV prevention.
Several key recommendations were outlined: include all stakeholders in a multidisciplinary national program; create a structured activities plan to increase awareness in the population; improve the quality of continuous CV health education; increase the interaction between different health professionals and non-health professionals; increment the referral of patients to cardiac rehabilitation; screen cholesterol levels in the general population, especially high-risk groups; promote patient self-care, engage with patients’ associations; use specific social networks to spread information widely; create a national database of cholesterol levels with systematic registry of CV events; redefine strategies based on the evaluation of results; create and involve more patients’ associations – invert the pyramid order.
In conclusion, ASCVD and the cholesterol burden remain a strong global issue in Portugal, requiring the involvement of multiple stakeholders in prevention. The Portuguese cholesterol roadmap can provide some solutions to help urgently mitigate the problem. Population-based approaches to improve awareness and CV risk assessment and surveillance of cholesterol and ASCVD outcomes are key factors in this change. A call to action is clearly needed to fight hypercholesterolemia and ASCVD burden.
A doença aterosclerótica cardiovascular (DACV) mantém-se a maior causa de morte prematura e de incapacidade, sendo uma prevenção eficaz de risco cardiovascular (CV) fundamental. O WHF Cholesterol Roadmap fornece enquadramento para o desenvolvimento de políticas nacionais, tendo como objetivo a prevenção de DACV. A convite da WHF, um grupo de peritos da Sociedade Portuguesa de Cardiologia (SPC) avaliou a carga do colesterol a nível nacional e discutiu possíveis estratégias para um Roadmap português.
A revisão da literatura mostrou uma carga elevada de colesterol em Portugal, sobretudo em pessoas de alto risco CV. Uma infografia, Scorecard, foi construída pela WHF, para mostrar claramente o risco CV e o peso do colesterol em Portugal, sendo útil para advocacia em políticas de saúde.
A discussão de peritos e proposta das estratégias preventivas seguiram os cinco pilares do documento da WHF: Melhoria da consciencialização; Abordagens do risco CV e do colesterol nas populações; Avaliação de risco/screening das populações; abordagens a nível do sistema; Seguimento do colesterol e complicações da DACV.
Várias recomendações chave foram definidas: incluir todos os stakeholders em programa multidisciplinar nacional; criar plano de atividades estruturadas para aumentar a consciencialização da população; aumentar qualidade da educação contínua em saúde CV; aumentar interação entre profissionais de saúde e outros profissionais; aumentar referenciação de doentes para reabilitação cardiovascular; avaliar níveis de colesterol na população geral, especialmente em alto risco; promover autocuidado dos doentes, envolvendo associações de doentes; usar redes sociais específicas para disseminar informação; criar base nacional de níveis de colesterol com registo sistemático de eventos CV; redefinir estratégias baseadas na avaliação de resultados; criar e envolver mais doentes em associações – inverter a ordem da pirâmide!
Em conclusão, a DACV e o peso de colesterol permanecem uma questão global forte em Portugal, necessitando o envolvimento de múltiplos stakeholders na prevenção. O Roadmap de colesterol português pode fornecer algumas soluções para urgentemente mitigar o problema. Abordagens a nível das populações para melhorar a consciencialização e avaliar o risco CV, seguimento do colesterol e das complicações de DACV são fatores chave nesta mudança. Uma call to action é claramente necessária para combater a carga da hipercolesterolemia e DACV.
Atherosclerotic cardiovascular diseases (ASCVD), including myocardial infarction, stroke, and peripheral arterial disease, remain major causes of premature death, disability, and healthcare expenditure globally.1 Cardiovascular risk and disease prevention strategies are crucial to reduce the associated mortality, morbidity and health costs across the world.
Advances in the current concepts of reducing cumulative exposure to cholesterol-containing lipoproteins and the emergence of novel therapies, provide new opportunities to improve prevention and decrease this burden of ASCVD.2 Healthcare strategies are needed to prevent ASCVD, including the avoidance of cholesterol-containing atherogenic lipoproteins accumulation in arterial walls.
The current World Heart Federation (WHF) Cholesterol Roadmap provides a conceptual framework for the development of national policies and health system approaches, so that potential obstacles to cholesterol management, and thus ASCVD prevention, can be adressed.2
Through a review of published guidelines and research papers since 2017, and consultation with a committee of experts in clinical management of dyslipidemia and health systems research in low-and-middle income countries, this roadmap identified:
- 1.
Key principles to effective ASCVD prevention.
- 2.
Gaps in implementation of these interventions (knowledge-practice gaps).
- 3.
Health system roadblocks for the treatment of elevated cholesterol in LMICs.
- 4.
Potential strategies for overcoming these gaps and limitations.
Reducing the burden of ASCVD requires multiple approaches throughout life: greater focus on primordial prevention; availability of affordable cholesterol testing; availability of universal cholesterol screening for inherited dyslipidemias; risk stratification moving from a 10-year risk to a lifetime risk, with adequate risk estimators; wider availability of affordable lipid-lowering therapies (LLT), which should include statins as global essential medications; use of whenever indicated high-intensity statin regimens; and combination therapies with ezetimibe or other drugs in order to achieving and maintaining robust reductions in low-density lipoprotein cholesterol (LDL-C) in those at highest risk. Continuing efforts are needed in health literacy for both public and healthcare providers, utilizing multidisciplinary teams in healthcare and applications that quantify ASCVD risk and the benefits of treatment, as well as increased adherence to therapies.
The document concludes that the adverse effects of LDL-C and apo B containing lipoprotein exposure are cumulative and result in ASCVD. These consequences are preventable by the implementation of different strategies aimed at efficiently tackling atherosclerosis at different stages throughout the course of life. Preventive strategies should therefore be updated to implement health policy, lifestyle changes, and when needed, earlier pharmacotherapies, with investment and shift in focus toward early preventive strategies, preserving CV health rather than treating the effects of ASCVD.
The WHF invited the National Societies to evaluate closely the problem of hypercholesterolemia in their individual countries, and inspired by the WHF Cholesterol Roadmap, to propose strategies to control hyperlipidemia and create a national roadmap. This article regards the production of a Portuguese cholesterol roadmap.
PurposeThe main purpose of this paper is:
- 1.
To evaluate the burden of hypercholesterolemia in Portugal in the last 10 years and to build a national infographic (scorecard), including cholesterol and other ASCVD risk factors, to be used for advocacy purposes and
- 2.
To propose preventive strategies to combat hypercholesterolemia in Portugal, helping to create a Portuguese cholesterol roadmap.
- 1.
A review of the literature regarding CVD and CV risk factors, in particular hypercholesterolemia, with creation of a national scorecard (infographic).
- 2.
A discussion of the strategies to control hypercholesterolemia in Portugal by a group of experts, helping to build a national roadmap.
The hypercholesterolemia burden in Portugal was identified and evaluated in a literature review over the last 10 years, creating the picture of hypercholesterolemia in Portugal, to be inserted in an infographic (scorecard).
The objective of the WHF's scorecard project is to create a clear picture of the current state of CV disease (CVD) prevention, CV risk factors (such as hypercholesterolemia) control and management in each country and feed it into a systemized assessment of CV policy on a regional and global scale. The advocates for heart health can improve the campaign to change the current reality if armed with a comprehensive overview of both the burden of CVD and the policies in place to tackle it. By measuring the national response to CVD, countries are better able to distinguish priorities, map progress, and ultimately, be held accountable for action to promote better outcomes.
A workshop was organized at the Portuguese Society of Cardiology (SPC), including experts in dyslipidemia, prevention, and public health. At this meeting, after the presentation of the WHF Roadmap by one of the authors, participants were grouped and discussed the focus of the WHF Cholesterol Roadmap:
- 1.
Awareness improvement strategies.
- 2.
Population-based approaches for CV risk and cholesterol decrease strategies.
- 3.
Risk assessment/population screening strategies.
- 4.
System-level approaches strategies.
- 5.
Surveillance of cholesterol and ASCVD outcomes strategies.
- 6.
Strategies proposed by the groups to combat this problem were then debated by all the participants in an idea generation workshop, with the goal of creating a national cholesterol roadmap to be used for advocacy and as a guide for CV prevention.
From the review of the relevant literature on the cholesterol problem in Portugal in the last 10 years, we now present the main results of the studies, registries, and guidelines in Portugal.
The VALSIM studyThe VALSIM study,3 published in 2013, included 16856 individuals (mean age 58.1±15.1 years), observed in primary healthcare centers in Portugal, which sought to characterize total cholesterol (TC), LDL-C, high-density lipoprotein cholesterol (HDL-C) and triglycerides (TG), showed a high prevalence of dyslipidemia in adults (62% female, 58±15 years). TC ≥200 mg/dl was recorded at 47% and LDL-C ≥130 mg/dl in 38% of the individuals analyzed. Hypertriglyceridemia (≥200 mg/dl) and low HDL-C (<40 mg/dl) were less prevalent, affecting 13% of the population. Hypercholesterolemia was particularly frequent in males aged 30–60 years, and in postmenopausal women, which should be target-subgroups for strategic public health strategies.
1st National Health Examination SurveyIn 2015, The National Health Institute Doctor Ricardo Jorge published the 1st National Health Examination Survey,4 as health questionnaires with a physical examination were a strategy from the European Commission to improve quality and to compare the quality of healthcare across Europe.
This survey was an epidemiologic observational transversal study with the main purpose of improving public health and decreasing inequities in Portugal. It examined a population of 4911 individuals aged 25–74 years old and included three components: physical examination, blood testing and clinical interview.
In summary, the main results were:
- •
52% of the Portuguese general population aged 25–74 years had TC ≥190 mg/dl.
- •
63% were taking medication to reduce cholesterol levels (no differences between male and female individuals).
- •
Prevalence of elevated TC or LLT increased with age, reaching 80% in individuals >55 years old.
- •
Prevalence of elevated TC or LLT was higher in central Portugal (74.4%) and lower in Lisbon and Tejo Valley (57.8%) (a trend that remained after standardization of prevalence according to age and gender).
In 2017, the Portuguese Directorate of Health (DGS) 2011 Norms were updated (the guidelines treatment on dyslipidemias, TC and TG target values and clinical audit instrument).5
EUROASPIRE IV and VIn Europe, the cross-sectional ESC-EORP EUROASPIRE Survey Registries IV6 and V,7 supported by the European Society of Cardiology (ESC), were conducted in patients with coronary atherosclerotic disease (CAD), to evaluate the implementation of CV prevention guidelines, which included lipid levels control and target values attainment. In the last EUROASPIRE V, 131 centers, from 81 geographical regions in 27 countries (including Portugal) enrolled 8261 patients between 2016 and 2017.
The summary and main conclusions of this study were7:
- •
71% of CAD patients had LDL-C level ≥70 mg/dl in Europe (mean value), while 69% in Portugal, with large differences among countries, ranging from 51% in Spain to 90% in Lithuania.
- •
37% of patients had LDL-C ≥100 mg/dl, 29% had never been informed of raised cholesterol, and 21% had not had any cholesterol measurements taken since hospital discharge.
- •
84% of patients were prescribed LLT, including 80% on statins and 50% on high-intensity statins or drug combinations (which may reduce LDL-C by >50%).
- •
32% of patients on LLT had LDL-C <70 mg/dl, although significantly less in female patients (p<0.0001); 76% reported full prescription compliance.
- •
29% of all CAD patients reported diabetes.
- •
46% were advised to participate in a cardiac rehabilitation program and 69% of those advised attended at least 50% of the sessions.
The results of the EUROASPIRE V survey showed that most CAD patients have less than optimal management of LDL-C. More professional strategies are needed, aiming at lifestyle changes and LLT adapted to the individual needs of the patient.
Another branch of EUROASPIRE was dedicated to evaluating CV risk in primary care (no CAD),8 of which the general results were:
- •
<50% patients on LLT achieving LDL-C target (better control in male patients).
- •
<50% patients on LLT were aware of their cholesterol levels and <33% knew their cholesterol target.
- •
>40% patients with elevated LDL-C had never been told they had high cholesterol.
The results of EUROASPIRE V are in accordance with earlier surveys of primary prevention in Europe, USA and worldwide, most of them focused on control of a single risk factor, while information on management of multiple risk factors in patients at high risk is limited.
The LATINO studyThe LATINO study,9 performed at 14 Portuguese health centers and one central hospital in the North of Portugal, included data from 78459 patients to evaluate lipid control in different CV risk groups. It identified major missed treatment opportunities to optimize LDLC management for every risk category, particularly emphasizing high- and very-high-risk patients. The higher the CV risk, the lower the number of patients with ideal targeted LDL-C:
- •
44% at low risk.
- •
27% at intermediate risk.
- •
7% at high risk.
- •
3% at very high risk.
This study also highlighted the need to use high-intensity statins and combination therapy, putting the most recent recommendations into clinical practice. Investment in adequate LDL-C control seems to be the most promising solution to decrease the high burden of ASCVD in Portugal.
Results II: Cholesterol and CV risk burden in Portugal - InfographicsThe objective of the scorecard project is to create a clear picture of the current state of CVD prevention, control, and management in each country, and feed it into a systemized assessment of CV policy on a regional and global scale. By measuring the national response to CVD, countries are better able to distinguish priorities, map progress, and ultimately, be held accountable for action to promote better outcomes.
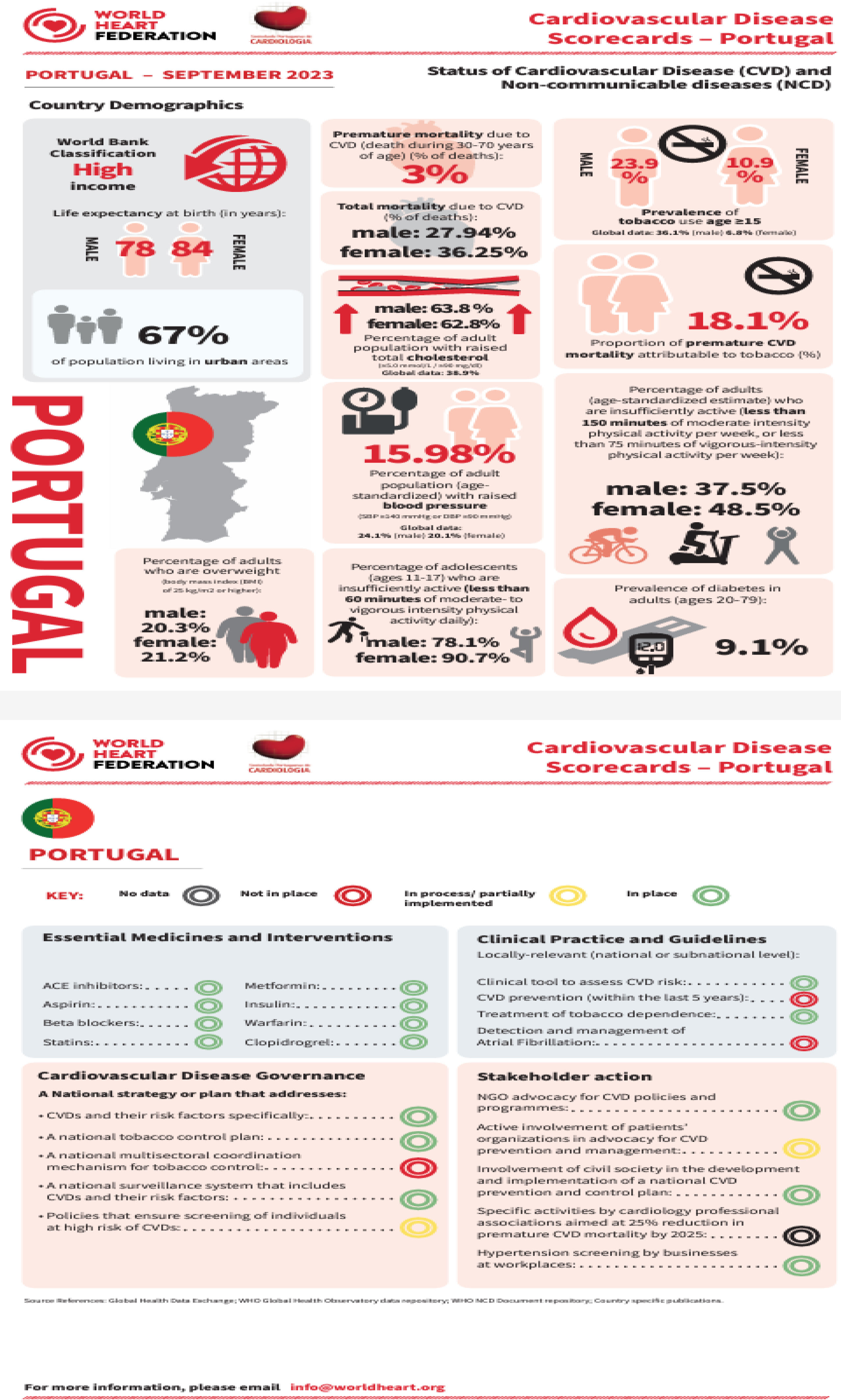
After the evaluation of Portuguese studies referring to cholesterol, and based on present data, a scorecard (infographic) was produced to be included in the WHF collection (Figure 2), for a clearer idea of the cholesterol burden and figures on other CV risk factors in Portugal (Figure 1) and also to gain knowledge on national pharmacological interventions in CV risk factors management, in Clinical practice and guidelines, strategies in CVD governance and stakeholder action (Figure 1).

Infographic: left side: premature mortality and CV risk factors including high cholesterol, hypertension, physical inactivity, smoking, diabetes in Portugal. Right side: essential medication and interventions for risk factor management, local relevant clinical practice and guidelines, national plans in CVD governance and stakeholder action.
Cardiovascular health advocates can improve campaigns to change the current scenario if they have a comprehensive overview of both the burden of CVD and hypercholesterolemia and the policies in place to tackle it.
DiscussionA roadmap is a clear and general strategic plan to achieve a particular target. Depending on the current situation – political, social, economic, religious, physical/psychological health, and literacy – strategies need to be designed and modified to adapt and achieve the target. In this setting, different countries will probably try to achieve the same targets, but with different barriers and starting points, sometimes using also different roads. The SPC was challenged to create a group of experts to generate ideas regarding potential solutions for the problem of inadequate cholesterol management. The main barriers for adequate management of the cholesterol in Portugal identified by the CV prevention experts were the lack of health literacy, low social-economic status, lack of good communication among stakeholders and lack of a structured plan.
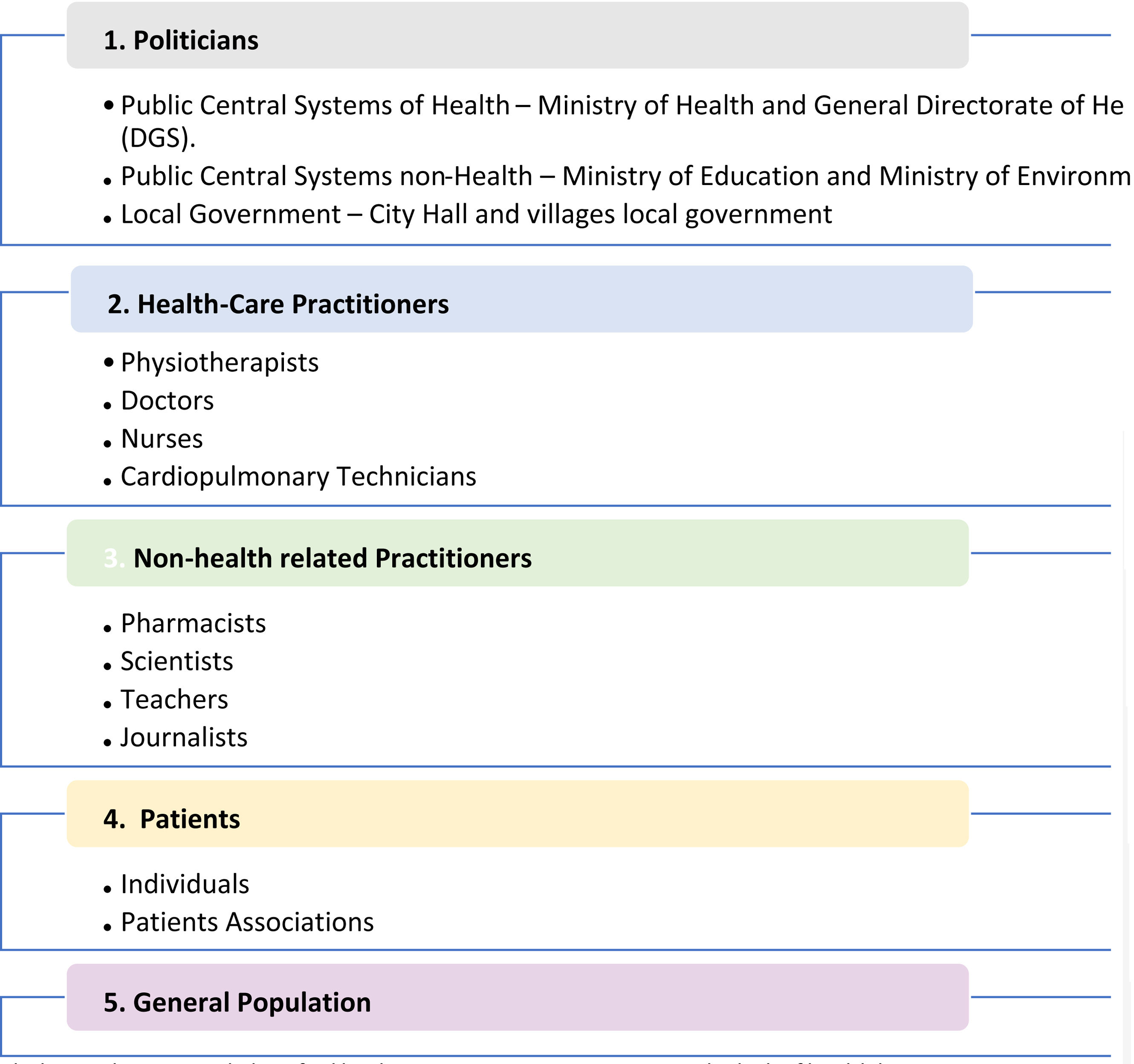
It was also emphasized that a national structured plan for cholesterol CV risk management involves different stakeholders identified in Figure 2. The place for action is very wide and can include ministries, city halls, hospitals, clinics, pharmacies, schools, universities, supermarkets, hairdressers, barbers, TV, radio, social networks, newspapers, and magazines.

The panel of experts decided a call for action was needed with strategies grouped according to the five main principles of the WHF Cholesterol Roadmap (Tables 1–5).
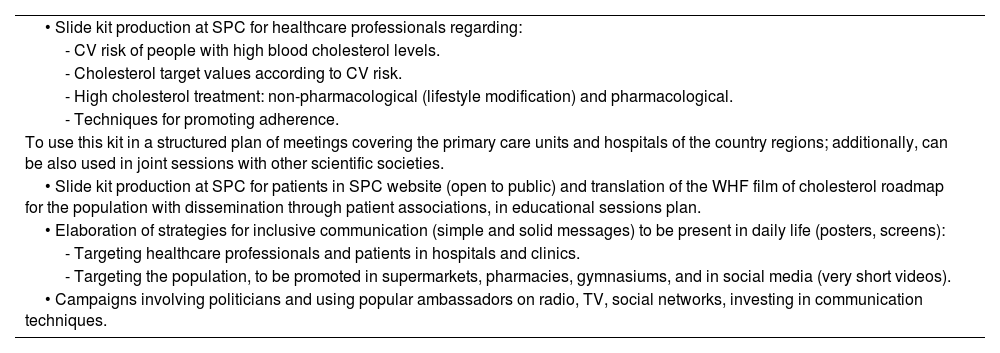
Awareness improvement strategies in the Portuguese cholesterol roadmap.
| • Slide kit production at SPC for healthcare professionals regarding: |
| - CV risk of people with high blood cholesterol levels. |
| - Cholesterol target values according to CV risk. |
| - High cholesterol treatment: non-pharmacological (lifestyle modification) and pharmacological. |
| - Techniques for promoting adherence. |
| To use this kit in a structured plan of meetings covering the primary care units and hospitals of the country regions; additionally, can be also used in joint sessions with other scientific societies. |
| • Slide kit production at SPC for patients in SPC website (open to public) and translation of the WHF film of cholesterol roadmap for the population with dissemination through patient associations, in educational sessions plan. |
| • Elaboration of strategies for inclusive communication (simple and solid messages) to be present in daily life (posters, screens): |
| - Targeting healthcare professionals and patients in hospitals and clinics. |
| - Targeting the population, to be promoted in supermarkets, pharmacies, gymnasiums, and in social media (very short videos). |
| • Campaigns involving politicians and using popular ambassadors on radio, TV, social networks, investing in communication techniques. |
Population-based approaches for CV risk and cholesterol decrease strategies in Portuguese cholesterol roadmap.
| • Convincing health politicians for legislation about food nutrients, reducing trans-fats. |
| • Mandatory introduction of codes (“traffic-light” like) in processed food, regarding the degree of healthy/non-healthy and the content of fats and trans-fats, and use of quality stamps. |
| • Educational actions at schools, from a very young age, on CV risk and high cholesterol risk, involving scientific societies and universities, with production of educational contents.10 |
| • Involvement of coffeehouses, restaurants and supermarkets in the reduction of fats intake, reduction of red meat, fat cheese, milk and butter and non-vegetable oils; with availability of a healthy menu scientifically supported by the national society. |
Risk assessment/population screening strategies in Portuguese cholesterol roadmap.
| • Calculation of digital risk scores in the population during big events or in big areas like malls or pharmacies, and education on CV risk, specially targeting those who are forgotten, like women11 and social minorities. |
| • Screening at schools for cholesterol level and education about healthy lifestyle, nutrition, and physical activity. |
| • Performance of National Questionnaire (2nd) with physical measurements, as per the first in 2015. |
System-level approach strategies in the Portuguese cholesterol roadmap.
| • Dissemination in different hospital/primary care units of CV risk scores and implementation of its use and education for it, using the risk level to guide CV management (preferably electronic version, available and transversal to different health institutions). |
| • Pressure at governmental level to reduce the price of statins and to make available new LLT in all hospitals (even more expensive ones), without inequalities. |
| • Promotion of affordable polypills to decrease CV risk and ASCVD burden to improve adherence and reduce CV events.12 |
| • Inclusion of CV risk and prevention education as mandatory in schools’ programs from a young age, though collaboration between Ministry of Health and Ministry of Education. |
| • Removal of uniform “normal values” of cholesterol from the blood test reports (values dependent on CV risk), and keep them up to date, according to the last guidelines. Also, the reporting of LDL cholesterol levels (calculated or measured) should be mandatory in blood tests reporting lipid profile. |
| • Increase referral for cardiac rehabilitation of CV patients after acute events (e.g. automatic referral in hospitals) and of high CV risk patients, even before events (signalizing high CV patients in primary care centers for referral). |
| • Promoting social health behaviors toward the media and local government structures like city halls, improving nutrition, physical activity, and places for wellbeing (gardens, tree planting in neighborhoods, low pollution), introducing practices for the population, such as yoga, dancing, gymnastic, stress management and relaxation techniques. |
Surveillance of cholesterol and ASCVD outcomes strategies.
| • Development of an anonymized national web based database for serial cholesterol quantitative levels and CV events sharing, with mandatory registration in all Hospitals and Primary Care Centers. |
| • Analysis of the Portuguese data of EUROASPIRE IV–V regarding the modification of cholesterol levels, management, and CV risk (data will be send from ESC to the Portuguese National Society). |
It was agreed that the problem of cholesterol is still a reality in Portugal. Despite all the efforts to reduce cholesterol levels, it was also pointed out that we must look more widely to the global risk profile, to the control of many CV risk factors, as smoking cessation, hypertension, obesity and diabetes, more than to isolated risk factors, promoting a healthy lifestyle, with physical activity and adequate nutrition, associated with drugs, as necessary, but mainly to forge different mentalities, with healthy behaviors and environments. In Portugal in 2019, data revealed that hyperglycemia, hypertension, smoking and high body mass index were more associated to coronary and cerebrovascular disease (main causes of death) than cholesterol. It is important to highlight that in the Portuguese cholesterol roadmap we are targeting the CV risk as a whole, despite our main concerns in this discussion having been the hypercholesterolemia burden.
The main points considered in this discussion, which should be part of a general plan to combat the problem, where the SPC can have a crucial role, are summarized as follows:
Recommendations: key points for action- •
Include all the stakeholders in a multidisciplinary and well conducted national program coordinated by Health National Services Task Force, including scientific societies, universities, associations, foundations, hospitals, and primary care centers, and prioritizing the value of patients’ associations with government's support.
- •
Create a structured activities plan to increase awareness of CVD and risk stratification (with cholesterol and other risk factors) in the population, with simple messages disseminated through competent and appropriate communication channels.
- •
Improve the quality of CV health education to healthcare professionals (which needs to be continuous), patients, public, politicians, journalists and especially children.
- •
Increase the interaction between different health professionals and with non-health professionals regarding ASCVD risk and cholesterol burden management.
- •
Increment referral of individuals with elevated CV risk and with already established CVD to cardiac rehabilitation.
- •
Screen the cholesterol levels (focus on LDL cholesterol levels) in general population, especially high-risk groups.
- •
Promote patients’ self-care, engaging patients’ associations to enhance CV risk and cholesterol management.
- •
Use specific social networks to spread information on CV risk and dyslipidemia and to educate healthcare professionals and the general population, reach a large range of people and increase health literacy.
- •
Create a national database with cholesterol levels and a systematic registry of CV events, accessible to all health units.
- •
Evaluate results and redefine strategies, as necessary, according to these results.
- •
Create and involve more patients’ associations – invert the pyramid order!
Some progress has already made regarding cholesterol prevention and management, with the intervention of the SPC, universities and the Portuguese Cardiology Foundation, highlighted in the activities listed below:
Work in progress: summary- •
ESC Preventive Guidelines translated to Portuguese by the SPC CV Risk Working Group.
- •
Multidisciplinary meeting for CV risk prevention implementation by the Institute of Preventive Medicine of the Faculty of Medicine of the University of Lisbon.
- •
CV risk and prevention strategies on health websites, TVs, newspapers, and social networks communication.
- •
CV prevention sessions in schools promoted by the SPC.
- •
Participation in radio programs about CV prevention promoted by the University of Lisbon.
- •
Questionnaire administered this year (2023) by the Portuguese Cardiology Foundation by phone to 800 Portuguese adults. From the inquired individuals, 88% (between 18 and 24 years old), 86% (between 25 and 44 years old), 66% (between 45 and 64 years old) and 69% (≥65 years old) did not know their cholesterol level. From these, 89% knew cholesterol is a circulating fat in the body and 64% indicated that the normal value is inferior to 190 mg/dl. Regarding the question which CVD were provoked by high cholesterol, 42% highlighted stroke, 25% myocardial infarction and 18% CVD. As the main cause of myocardial infarction, 49% pointed out high cholesterol and 32% hypertension.
The SPC, particularly its CV Risk Working Group, is engaged in fighting the cholesterol and global ASCVD risk burden with the WHF and European Societies and Associations, defining strategies for cholesterol control and global CV risk management. A national survey on CV risk with appropriate analysis and follow-up could be a way of monitoring this situation and insisting on action by politicians, which may be part of the solution.
ConclusionsCholesterol management remains a global strong issue for both primary and secondary prevention, also in Portugal. The involvement of multiple stakeholders, including politicians, healthcare practitioners, non-health-related practitioners, patients, and the general population, is essential to overcome current limitations in this field. The Portuguese cholesterol roadmap, which arose from the idea generation promoted by the WHF at the SPC involving cardiologists and other specialists, can provide some solutions to urgently help minimize this problem. Population-based approaches to improve awareness and strategies for CV risk assessment, surveillance of cholesterol and ASCVD outcomes, are key factors in this change. A call to action is clearly needed to fight hypercholesterolemia and ASCVD burden.
FundingWHF funded Portuguese Society of Cardiology expert work regarding the Portuguese Cholesterol Roadmap.
Conflicts of interestThe authors have no conflicts of interest to declare.
