




A 22-year-old male was admitted to the emergency room due to a left hemithorax injury from a screwdriver (Figure 1A). The patient was hemodynamically stable, with a slightly altered mental status. Chest computed tomography was performed and revealed moderate pericardial effusion, leading to an evaluation by the cardiology emergency team. The transthoracic echocardiogram revealed severe aortic valve regurgitation, raising suspicion of aortic root injury, as well as fistulous communications between heart chambers (Figure 1B–D). These findings led to emergent surgery.
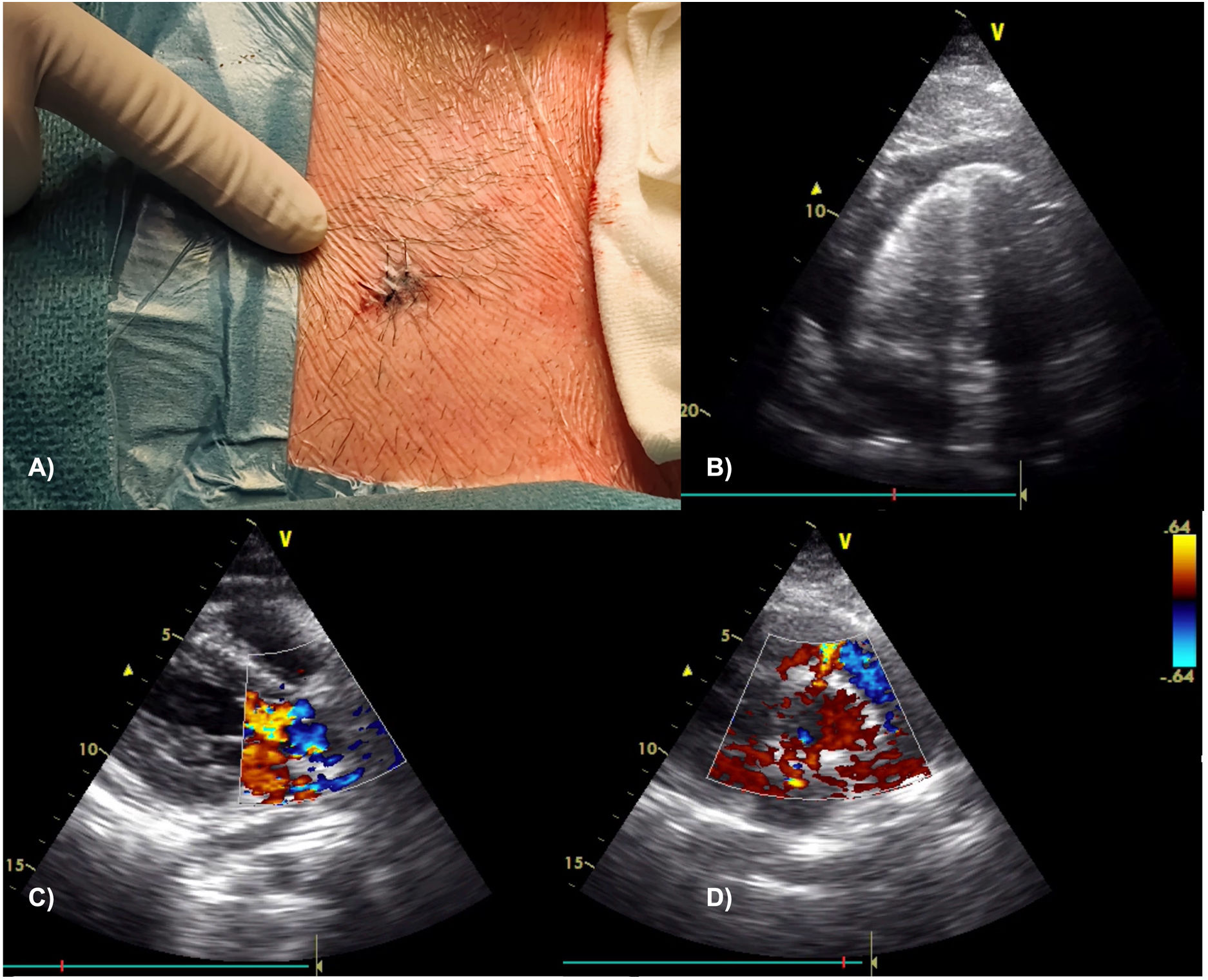
Chest wall lesion (A) and transthoracic echocardiographic images showing a circumferential and large pericardial effusion (B), as well as turbulent flow in aortic root and a severe aortic valve regurgitation (C); fistulous communications between both the right ventricle and left atrium to the aortic root were suspected in the parasternal short axis view (D).
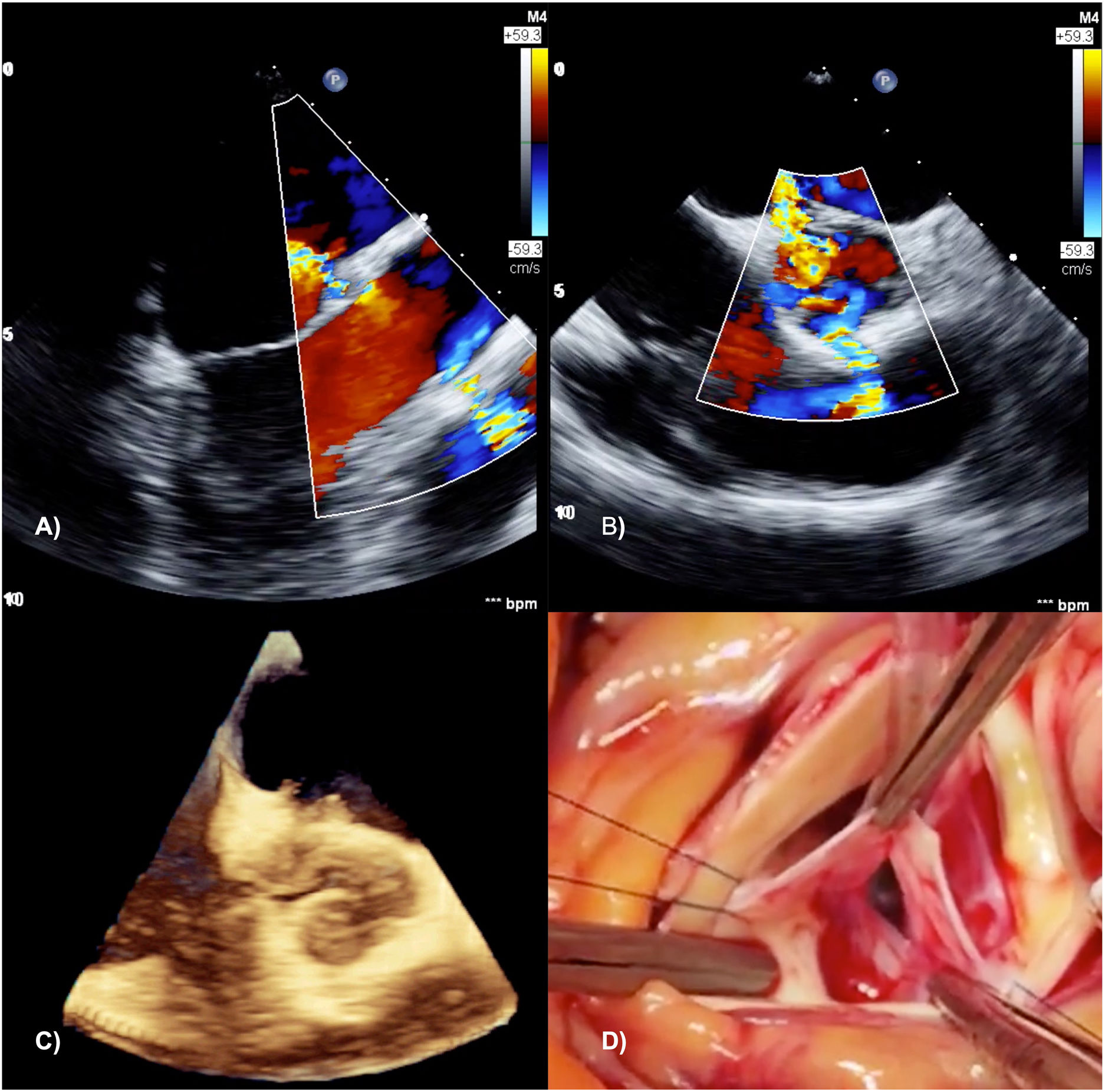
Intraoperative transesophageal echocardiogram images confirmed an injury path originating in the right ventricle, crossing the aortic valve root, and ending in the left atrium (Figure 2A–C). An aortic valve replacement, closure of the aortic root fistulas and infundibular lesion were performed (Figure 2D). The patient had excellent postoperative recovery and was discharged after six days.
Our case reports an apparently stable patient despite worrisome echocardiographic findings, especially traumatic valve injury, which is a rarely reported lesion.1 It is an astonishing case due to a lucky (millimetric) save from an open aortic injury, which is fatal in most cases.2
We emphasize the high mortality rates associated with penetrating cardiac injury3 and the importance of keeping a high index of suspicion for these lesions after chest trauma.3
Furthermore, we underline how stab injuries may present with subtle imaging findings,2 hindering their recognition and justifying the crucial role of cardiac imaging for early diagnosis and correct management.3,4
Conflicts of interestThe authors have no conflicts of interest to declare.
