



Pericardial cysts are rare and generally benign intrathoracic lesions, most frequently located in the cardiophrenic angles, but other locations have been described. We present a case of a pericardial cyst in a previously undescribed site. Our patient presented with a cyst in the interventricular septum which was discovered as an incidental finding. After surgical excision of the cyst, it was described pathologically as a simple mesothelial pericardial cyst. The explanation of this rare condition is uncertain, but some hypotheses can be outlined.
Os cistos pericárdicos são lesões intratorácicas raras e geralmente benignas, mais frequentemente localizadas nos ângulos cardiofrénicos, no entanto, outras localizações têm sido descritas. Apresentamos o caso de um cisto pericárdico num local não descrito previamente. O nosso doente apresentou-se com um cisto no septo interventricular que foi detetado como achado incidental. Após a excisão cirúrgica do cisto, este foi descrito anatomopatologicamente como um cisto pericárdico mesotelial simples. A explicação para esta localização incomum é incerta, mas algumas hipóteses podem ser delineadas.
Congenital pericardial cysts are rare and benign intrathoracic lesions.1,2 The preferential location is in the cardiophrenic angles,1 but other unusual locations have been described. We present a case of a pericardial cyst in a particularly uncommon location.
Case reportA 39-year-old man was referred for evaluation of an intracardiac mass. His past medical history was irrelevant except for allergic rhinitis. He worked in the environmental department of the National Republican Guard, and was thus frequently in contact with animals. There was no relevant travel abroad, consumption of potentially hazardous foods, or alcohol or drug abuse.
Regarding family history, his mother was diagnosed with systemic hypertension in her twenties and was being followed for suspected aortic dilatation and cardiac valve disease. His father also had hypertension.
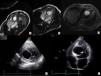
The patient was asymptomatic and underwent routine exams, including an electrocardiogram which revealed nonspecific abnormalities due to which he was referred for a transthoracic echocardiogram (TTE). This showed an intracardiac cystic mass. A transesophageal echocardiogram (TEE) and additional blood tests were performed. The latter only revealed eosinophilia of 3.1%, while the former confirmed the presence of a cystic mass with a diameter of 4.5 cm located in the interventricular septum, protruding into the left ventricular outflow tract and extending to 1 cm below the aortic valve, with associated septal hypokinesia, and without continuity with the cardiac chambers. A bicuspid aortic valve with moderate aortic regurgitation and a dilated ascending aorta were also observed. Magnetic resonance imaging (MRI) showed the mass to be hyperintense in T2, revealed moderate aortic regurgitation and confirmed the other echocardiographic findings (Figure 1). The patient was asymptomatic.
He was then referred for cardiac surgery evaluation, and underwent a new TTE in our hospital, which confirmed the previous findings. The case was discussed and accepted for surgery.
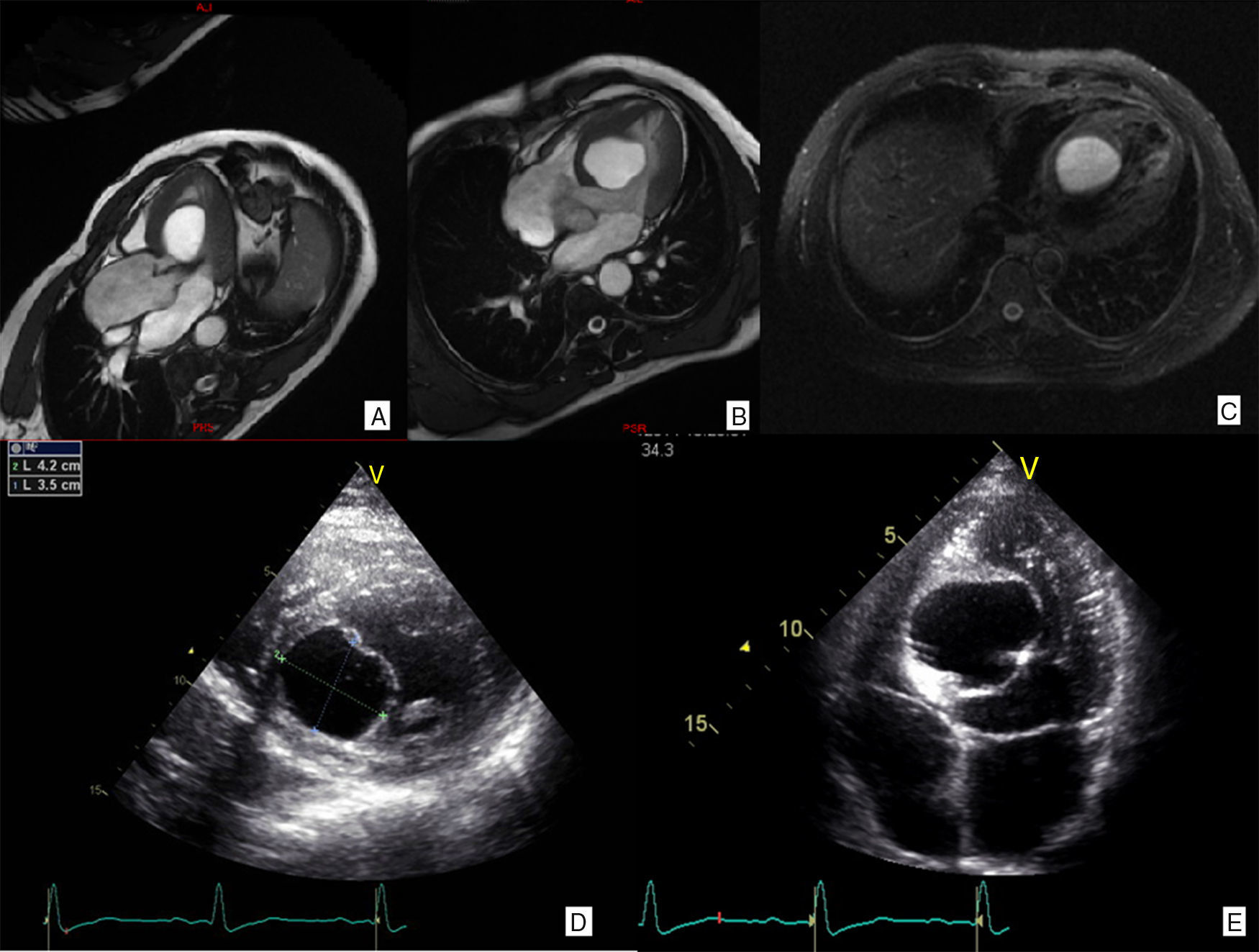
The patient underwent surgery, the cyst being excised through enucleation by blunt dissection with (at times unsuccessful) attempts to preserve the capsule (Figure 2A-C) plus aortic valve replacement with a mechanical valve (27 mm St. Jude Medical Regent®). The ascending proximal aorta and the aortic root (noncoronary sinus) were replaced with a 28 mm Gelseal® graft by a modified Bentall procedure. There were no complications during surgery. The postoperative echocardiogram showed that the inferior part of the septum was thin and dyskinetic, but there were no other abnormalities. The patient was discharged 10 days after surgery (Figure 2D-E).
(A-C): Images captured during surgical resection of the cyst. (A): Cyst causing bulging of the interventricular septum and protruding into the left ventricular outflow tract; (B): intramyocardial location of the cyst; (C): cyst rupture and flow of clear fluid; (D and E): transthoracic echocardiogram after surgery showing a thin interventricular septum and delineation of the previous location of the cyst; (F and G): microscopic aspects of the cyst: (F): cyst wall, H & E stain ×100; (G): cytokeratin 5/6 ×400 (left) and vimentin ×400 (right): keratin and vimentin co-expression by the cells of the internal layer of the cyst. RE: internal cell layer of the cyst; F: fibrosis; M: myocardium.
Pathological examination of the cyst revealed that macroscopically it was a cystic formation 4 cm in its largest diameter and microscopically a cyst with a sheath composed of a single cell layer, positive for keratin and vimentin. The wall was thin and fibrous with focal and scattered calcifications and in continuity with the adjacent myocardium. The diagnosis was a simple mesothelial pericardial cyst (Figure 2F-G).
DiscussionCongenital pericardial cysts occur in 1/100000 individuals and account for 7% of mediastinal masses.1 Pericardial cysts are usually detected in middle-aged adults.2
Pericardial cysts are commonly located in the left (51-70%) and right (28-38%) cardiophrenic angles and a small percentage are located in the upper mediastinum, hilum or cardiac border.1
In this case, the cyst was diagnosed in the fourth decade of life. To our knowledge, this is the first reported case of a pericardial cyst with an intramyocardial location.
Congenital pericardial cysts arise when a portion of the pericardium pinches off during embryonic development.1 Lambert proposed a new causal concept, the “lacuna theory”, suggesting that cysts derive from disconnected mesenchymal lacunae, which later unite to form the pericardial cavity. Failure of one of these lacunae to merge with the others would result in the formation of a congenital cyst.3,4
Wessels and Pérez-Pomares5 draw attention to the transmural migration and differentiation pathways of epicardially derived cells, which act as cardiac stem cells. Such cellular behavior could explain unusual intracardiac, including intramyocardial, locations of pericardial cysts, as in our patient.
The classic description of a pericardial cyst is a unilocular, smooth-walled cyst with an outer layer of endothelial or mesothelial cells. Their serous fluid-filled center and lack of solidity distinguishes them from other pericardial masses.1,2
The majority of pericardial cysts are asymptomatic, but they can cause symptoms of dyspnea, thoracic pain, and cough.2
Pericardial cysts are usually incidental findings, appearing as a round mass on chest radiography or as a homogeneous echolucent mass on TTE.1 TEE can be useful if TTE is insufficient to establish the diagnosis.2 On MRI their contents are hyperintense on T2-weighted images and hypointense on T1-weighted images.1
The diagnosis of pericardial cysts is not always straightforward since they may present in atypical locations. Furthermore, neither of the available non-invasive imaging modalities is sufficiently reliable to differentiate pericardial cysts from other pericardial masses with similar appearances but with different prognosis and treatments.1
The differential diagnosis should take into consideration solid tumors,2 hydatid cysts and mesotheliomas.
This patient denied any symptoms and the cyst was an incidental finding. None of the imaging exams performed aided in establishing the correct diagnosis, probably due to the extremely unlikely location, although the imaging description corresponded largely to that of a pericardial cyst. The main differential diagnosis considered before surgery was hydatid cyst, due to the patient's occupational background, local epidemiology and eosinophilia. The latter could have been related to allergic rhinitis.
Rarely, pericardial cysts can have a complicated course with rupture, erosion into adjacent structures, cardiac tamponade, and even sudden death.2
The management of pericardial cysts may be conservative or surgical, or involve percutaneous aspiration. Surgical resection is widely accepted as the treatment of choice when a patient has symptoms related to a mediastinal mass or if the diagnosis is uncertain.2
Due to the patient's indication for surgical treatment for aortic ectasia and bicuspid aortic valve disease, the cyst was resected concomitantly. The suspicion of a hydatid cyst was an additional motive for excision, due to the risk of rupture and consequent anaphylaxis.
In conclusion, to the best of our knowledge this is probably the first description of an intramyocardial pericardial cyst. The explanation for this unexpected location is uncertain, despite the above-mentioned evidence and theories. This case indicates the need to consider alternative diagnoses, even if in an unlikely location.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
The authors wish to thank Carlos Aguiar, MD, for helping in the revision of the manuscript.
