





Differentiation of ischemic from non-ischemic etiology in heart failure (HF) patients has both therapeutic and prognostic implications. One possible approach to this differentiation is direct visualization of the coronary tree. Multidetector computed tomography (MDCT) has emerged as an alternative to invasive coronary angiography (ICA), but its performance and additional clinical value are still not well validated in patients with left ventricular (LV) dysfunction. We aimed to assess the value of coronary MDCT angiography (CTA) in the exclusion of ischemic etiology in HF patients and to determine whether the Agatston calcium score could be used as a gatekeeper for CTA in this context.
MethodsWe retrospectively selected symptomatic HF patients with LV ejection fraction (LVEF) <50%, as assessed by echocardiography, referred for CTA between April 2006 and May 2013. Patients with previously known CAD or valvular disease were excluded. The performance of MDCT in the detection of coronary artery disease (CAD) and/or exclusion of an ischemic etiology for HF was studied. Obstructive CAD was defined as the presence of ≥50% luminal stenosis in at least one epicardial coronary artery as assessed by CTA and was assumed in patients with an Agatston coronary artery calcium (CAC) score >400. In patients referred for ICA, an ischemic etiology was assumed in the presence of ≥75% stenosis in two or more epicardial vessels or ≥75% stenosis in the left main or proximal left anterior descending artery.
ResultsDuring this period 100 patients (mean age 57.3±10.5 years, 64% men) with HF and systolic dysfunction were referred for MDCT to exclude CAD. Median effective radiation dose was 4.8 mSv (interquartile range 5.8 mSv). Mean LVEF was 35±7.7% (range 20-48%) and median CAC score was 13 (interquartile range 212). Seven patients were in atrial fibrillation.
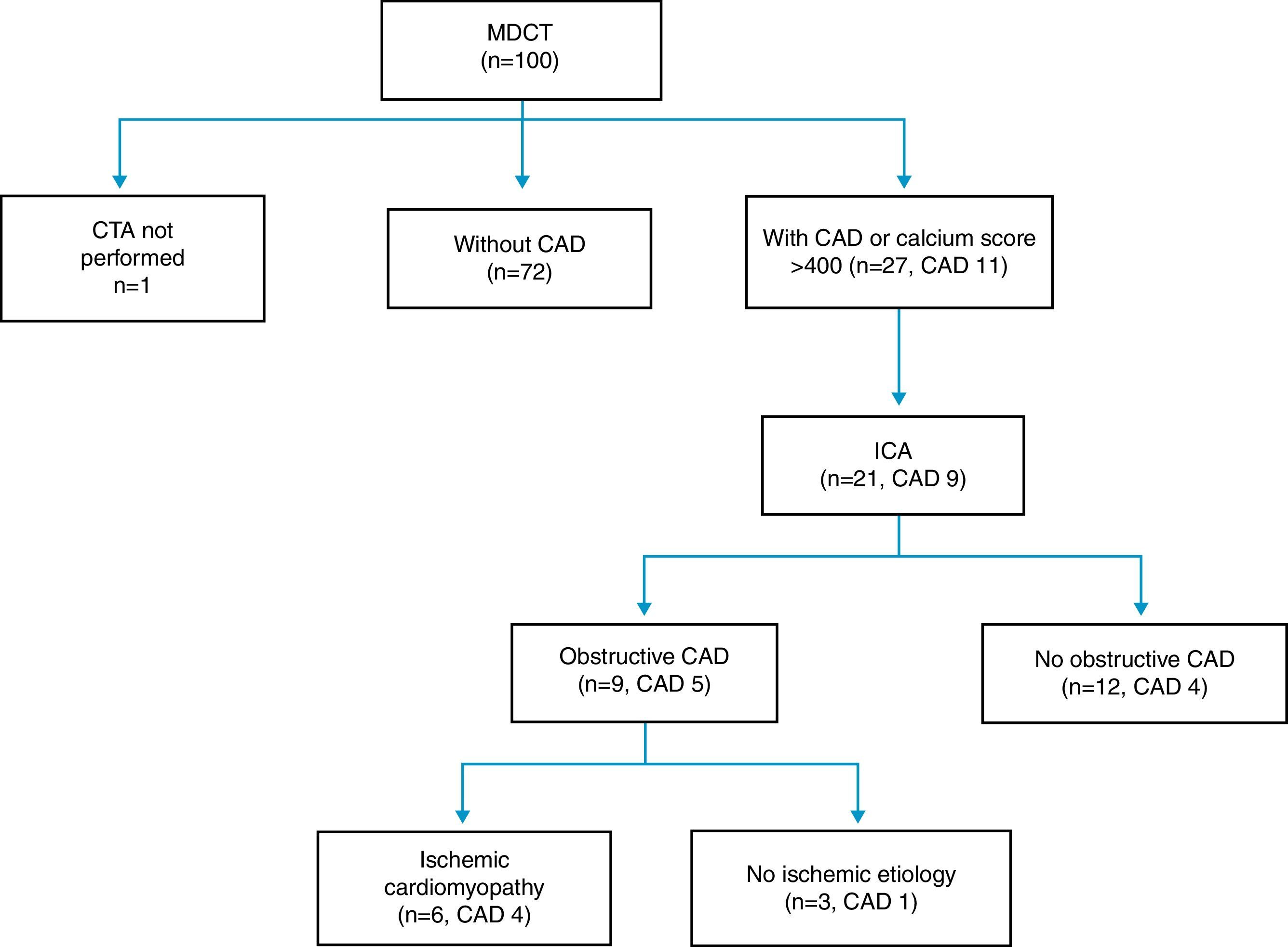
Almost half of the patients (40%) had no CAC and none of these had significant stenosis on CTA. In an additional group of 33 patients CTA was able to confidently exclude obstructive CAD. Twenty-seven patients were classified as positive for CAD (16 due to CAC >400 and 11 with ≥50% stenosis) and were associated with lower LVEF (p=0.004). Of these, 21 patients subsequently underwent ICA: obstructive CAD was confirmed in nine and only six had criteria for ischemic cardiomyopathy.
ConclusionIn our HF population, MDCT was able to exclude an ischemic etiology in 73% of cases in a single test. According to our results the Agatston calcium score may serve as a gatekeeper for CTA in patients with HF, with a calcium score of zero confidently excluding an ischemic etiology.
A diferenciação entre etiologia isquémica de etiologia não-isquémica em pacientes com insuficiência cardíaca (IC) tem implicações terapêuticas e prognósticas. Uma abordagem possível para esta diferenciação é a visualização direta da árvore coronária. A tomografia computorizada (TC) surgiu como uma alternativa à angiografia coronária, mas o seu desempenho e valor clínico adicional ainda não se encontram validados em pacientes com disfunção do ventrículo esquerdo. O nosso objetivo foi avaliar o papel da angio-TC coronária na exclusão de etiologia isquémica em pacientes com IC e avaliar se o score e cálcio Agatston pode ser usado como gatekeeper para a angio-TC coronária neste contexto.
MétodosForam selecionados retrospetivamente pacientes com IC sintomática com fração de ejeção do ventrículo esquerdo (FEVE)<50%, avaliada por ecocardiografia, referenciados para realização de angio-TC coronária entre abril de 2006 a maio de 2013. Pacientes com doença arterial coronária (DAC) ou doença valvular foram excluídos. Foi avaliado o desempenho da TC na deteção de DAC e/ou exclusão de etiologia isquémica. A DAC obstrutiva foi definida pela presença de estenoses luminais ≥50% em pelo menos uma artéria coronária epicárdica, avaliada por angio-TC coronária e foi assumida em pacientes com o score de cálcio Agatston >400. Nos pacientes referenciados para angiografia coronaria, a etiologia isquémica foi assumida na presença de estenoses ≥75% em duas ou mais artérias epicárdicas ou ≥75% no tronco comum ou no segmento proximal da artéria descendente anterior.
ResultadosDurante este período, 100 pacientes (idade média: 57,3±10,5 anos, 64% homens) com IC e disfunção sistólica foram referenciados para TC para exclusão de DAC. A dose mediana de radiação efetiva foi de 4,8 mSv (intervalo interquartil 5,8 mSv). A FEVE média foi de 35±7,7% (intervalo 20-48%) e a mediana de score de cálcio Agatston foi de 13 (intervalo interquartil 212). Sete pacientes apresentavam fibrilhação auricular.
Quase metade dos pacientes (40%) não apresentava score de cálcio e nenhum deles apresentava uma estenose significativa na angio-TAC coronária. A angio-TC coronária foi capaz de excluir DAC obstrutiva num outro grupo de 33 doentes. Vinte e sete pacientes foram classificados como positivos para a presença de DAC (16 através do score de cálcio Agatston>400 e 11 apresentavam estenoses≥50%) e foram associados a uma menor FEVE (p=0,004). Destes, 21 pacientes realizaram angiografia coronária: em 9 foi confirmada a presença de DAC obstrutiva e apenas seis apresentavam critérios para cardiomiopatia isquémica.
ConclusõesNa nossa população com IC, a TC foi capaz de excluir uma etiologia isquémia em 73% dos casos com um único teste. De acordo com os nossos resultados, o score de cálcio Agatston pode servir como gatekeeper para a angio-TAC coronária em pacientes com IC, com um score de cálcio de 0 a excluir confiadamente uma etiologia isquémica em pacientes com IC.
Heart failure (HF) is a complex and progressive disease that leads to significant morbidity and mortality. Approximately 1-2% of the adult population in developed countries has HF, the prevalence rising to ≥10% among persons aged 70 years or older.1 There are many causes of HF, and these vary in different parts of the world. However, the etiology is routinely categorized as ischemic or non-ischemic.
Patients with ischemic HF may benefit from revascularization2 and so the presence, anatomic characteristics, and functional significance of coronary artery disease (CAD) should be assessed in patients with new-onset HF.3
The gold standard diagnostic method for CAD detection has been invasive coronary angiography (ICA). Multidetector computed tomography (MDCT) has emerged as a robust alternative, demonstrating high diagnostic performance for identifying coronary stenosis.4 Several recent studies5–8 have shown that it is extremely accurate even in subjects with left ventricular (LV) dysfunction. Therefore, new-onset HF is currently considered an appropriate indication for MDCT.9 However, the performance of coronary MDCT angiography (CTA) for the differentiation of HF etiology in clinical practice has not been fully validated, and few studies have set out to evaluate the role of coronary artery calcium (CAC) score and CTA in patients with LV dysfunction. We sought to assess the value of MDCT in the exclusion of ischemic etiology in HF patients and to test the potential application of the Agatston score as a gatekeeper for CTA in this context.
MethodsStudy populationBetween April 2006 and May 2013, 4424 patients underwent cardiac computed tomography (CT) for detection of CAD. Of these we retrospectively selected patients with symptoms and/or signs of HF and systolic dysfunction (defined as left ventricular ejection fraction [LVEF] <50%) who were referred for CTA aiming to exclude an ischemic etiology.10 Subjects with previously known CAD or severe valvular disease were excluded from the analysis.
Patient preparationPatients received oral metoprolol one hour before the MDCT scan according to baseline heart rate (50 mg if >55 and <65 bpm or 100 mg if ≥65 bpm). An additional dose of intravenous metoprolol (2.5–15 mg) was administered 10 minutes before the scan if heart rate remained >65 bpm. All patients received 0.5 mg of sublingual nitroglycerin five minutes before CTA. Beta-blockers were not given in patients with class III/IV heart failure symptoms.
Assessment of pre-test probability for obstructive coronary artery diseaseA modified Morise risk score11 with exclusion of estrogen status was used to stratify the pre-test risk. Patients were classified as low (score <10), intermediate (10-16) or high (>16) pre-test probability, according to this risk score.
Scan protocolAll scans were performed using a 64-slice CT scanner (SOMATOM Sensation 64, Siemens Medical Solutions, Forchheim, Germany).
Agatston calcium score quantificationAll patients underwent a low-dose scan to assess CAC. The scan parameters for this acquisition were collimation 24×1.2 mm, gantry rotation time 330 ms, pitch 0.2, tube voltage 120 kV and tube current 190 mAs. Image reconstruction of the calcium score acquisition was performed using an effective slice thickness of 3 mm. CAC was reported as the mean Agatston score and was calculated using a detection of 130 HU with semi-automated software (syngo Calcium Scoring, Siemens Medical Solutions) as described previously.12
CAD assessmentIn patients with CAC ≤400, a CTA acquisition was performed (collimation 64×0.6 mm; tube current 850 mAs; all other parameters as in the CAC acquisition scan, with the exception of tube voltage, which was reduced to 100 kV in lower weight patients, according to the radiographer's judgment). Tube current modulation with electrocardiographic pulsing was used to decrease the radiation dose, with full tube current applied at 60–65% of the RR interval. Depending on the scan time, a bolus of 50–90 ml of contrast (Ultravist®, iopromide 370 mg/ml, Bayer Schering Pharma AG, Berlin, Germany) was injected (4.5–7 ml/min) via a power injector (Stellant® D, Medrad Inc., Warrendale, PA, USA) followed by a 40-ml saline chaser, using a dedicated antecubital vein 18-gauge access catheter. A bolus-tracking technique was used, with a region of interest placed in the ascending aorta, set to detect a predefined threshold of 150 HU. For assessment of CAD, multiphase sets of the reconstructed CTA images were processed on a dedicated workstation and analyzed for detection of at least one luminal diameter narrowing of >50% in any coronary artery segment.13 Severely calcified segments (concentric vessel wall calcification precluding lumen assessment) were classified as positive for CAD. Following the center's protocol and international consensus,9 CTA was not performed in patients with an Agatston calcium score higher than 400. These patients were considered positive for the presence of CAD.9,12,14,15
Radiation exposureMean radiation exposure was estimated by the method proposed by the European Working Group for guidelines on quality criteria in CT.16 The effective radiation doses for the CAC and CTA acquisitions were calculated by the product of the conversion coefficient for cardiac CT (0.014 mSv/mGy cm averaged between male and female models) and the dose-length product obtained during each scan.16
Image diagnostic qualityImage quality was subjectively classified by the readers into three groups: good, average and poor.
All tests were taken into consideration assuming an intention to diagnose and no patients were excluded from analysis based on image quality. Non-diagnostic segments due to poor image quality were assumed positive for CAD for the purposes of the study.
Invasive coronary angiography and ischemia testingPatients were referred for ICA and non-invasive ischemia testing at the referring physician's discretion. Data from tests performed in the 12 months after the exam were described.
For ICA, the same cut-off values described for CTA were used: coronary artery obstruction was defined as ≥50% luminal stenosis in at least one major coronary artery. An anatomically-based definition for ischemic cardiomyopathy on ICA was taken as ≥75% stenosis in the left main or proximal left anterior descending artery or in ≥2 epicardial vessels.17
Statistical analysisStatistical analyses were performed using SPSS 17.0 (IBM, Chicago, IL) and statistical significance was defined as p<0.05. Categorical variables were presented as frequencies with percentages. Continuous variables were presented as means ± standard deviations (SD) if normally distributed or as medians (interquartile range [IQR]) if non-normally distributed. For patient characteristics and imaging parameters, Fisher's exact test was used to compare categorical variables, and the Student's t test or the Mann-Whitney test were used for continuous variables.
ResultsOf the 4424 patients who underwent CTA between April 2006 and May 2013, 100 fulfilled the study's inclusion criteria. Patient data are presented in Table 1.
Baseline characteristics, pre-test risk score, scan protocol data, left ventricular ejection fraction and Agatston calcium score of the general population and patients with or without obstructive coronary artery disease as assessed by multidetector computed tomography.
| General population (n=100) | Without obstructive CAD (n=73) | Obstructive CAD or CACS >400 (n=27, 11 CAD) | p | |
| Age, years (mean ± SD) | 57.3±10.5 | 57.0±11.1 | 58.3±8.8 | 0.57 |
| Male, % | 64.0 | 60.3 | 74.1 | 0.20 |
| BMI, kg/m2(mean ± SD) | 27.0±4.7 | 27.7±4.9 | 25.1±3.1 | 0.01 |
| Hypertension, % | 55.0 | 57.5 | 48.1 | 0.40 |
| Diabetes, % | 14.0 | 13.7 | 14.8 | 0.89 |
| Obesity, % | 22 | 26.0 | 11.1 | 0.12 |
| Hyperlipidemia, % | 42.0 | 38.4 | 51.9 | 0.23 |
| Smoking, % | 27.0 | 23.3 | 37.0 | 0.17 |
| Family history, % | 13.0 | 13.7 | 11.1 | 0.73 |
| Modified Morise risk score | ||||
| Morise risk score, mean ± SD | 10.2±2.4 | 10.1±2.6 | 10.4±2.0 | 0.56 |
| Low, % | 26 | 28.8 | 18.5 | 0.47 |
| Intermediate, % | 72 | 69.9 | 77.8 | |
| High, % | 2 | 1.4 | 3.7 | |
| Maximum SBP, mmHg (mean ± SD) | 132.3±18.4 | 133.5±18.8 | 127.7±17.1 | 0.36 |
| Minimum SBP, mmHg (mean ± SD) | 78.2±11.7 | 77.8±12.1 | 79.7±10.5 | 0.62 |
| Heart rate, bpm (median, IQR) | 64.0 (11.8) | 64.0 (15) | 70.5 (22) | 0.52 |
| Atrial fibrillation, % | 7 | 5.5 | 11.1 | 0.33 |
| Beta-blockers, % | 69 | 72 | 60 | 0.27 |
| Effective radiation dose, mSv (median, IQR) | 4.8 (5.8) | 5.5 (5.1) | 0.9 (9.4) | 0.005 |
| LVEF, % (mean ± SD) | 35±7.7 | 37±7.0 | 31±8.3 | 0.004 |
| Agatston calcium score, median (IQR) | 13 (212) | 0.0 (10) | 229 (1359) | <0.001 |
BMI: body mass index; CACS: coronary artery calcium score; CAD: coronary artery disease; IQR: interquartile range; LVEF: left ventricular ejection fraction; SBP: systolic blood pressure.
Diagnostic quality of CTA was classified as good in 67% of patients, average in 25% and poor in 8%.
According to the MDCT findings, 27 patients presented obstructive CAD: 11 with ≥50% luminal stenosis and 16 with CAC >400 (Figure 1).
Patients with obstructive CAD presented lower body mass index (25.1 vs. 27.7 kg/m2, p=0.01), less radiation exposure (following the study protocol) (0.9 vs. 5.5 mSv, p=0.005) and lower LVEF (31 vs. 37%, p=0.004).
All patients with obstructive CAD as assessed by CTA had some degree of calcification (CAC >0) and the patient with the lowest calcium score in this group had a value of 3.3.
Of the 27 patients with CAD as assessed by MDCT, 21 underwent ICA (nine with CAD according to CTA and 12 with Agatston calcium score >400). Six patients with CAD detected on MDCT did not undergo ICA. Of these, two were referred for non-invasive stress perfusion imaging and ischemia was excluded. In the other four patients the physician's decision was to correct cardiovascular risk factors and to optimize therapy without further testing.
Of the 21 patients who underwent ICA, 12 had non-obstructive CAD and nine (43%) had obstructive CAD. Of these only six (29%) had criteria for ischemic cardiomyopathy (Table 2).
Results of multidetector computed tomography coronary angiography and Agatston calcium score in patients with obstructive coronary artery disease on invasive coronary angiography.
| Patients with obstructive CAD on ICA | CAD on CTA | Agatston calcium score >400 | Ischemic cardiomyopathy | Calcium score |
| 1 | + | – | – | 312.3 |
| 2 | + | – | + | 305 |
| 3 | – | + | – | 1227 |
| 4 | – | + | – | 1221.2 |
| 5 | + | – | + | 16.9 |
| 6 | – | + | + | 1155 |
| 7 | + | – | + | 30.3 |
| 8 | + | – | + | 152 |
| 9 | – | + | + | 868 |
CAD: coronary artery disease; CTA: multidetector computed tomography coronary angiography; ICA: invasive coronary angiography.
Of the seven patients in atrial fibrillation (AF), one had tachycardia precluding CTA acquisition and only underwent CAC testing. Of the remaining six, three had no CAD, one had ≥50% stenosis on CTA and two had CAC >400. Average image quality was reported in all of these CTA cases. The patient with rapid heart rate and the patients with obstructive CAD and CAC >400 underwent ICA, which revealed no obstructive CAD.
DiscussionThe main finding of our study is that in symptomatic heart failure patients with depressed LV function of unknown etiology, MDCT was able to exclude CAD in the majority of cases (73%). Furthermore, in our intermediate to low pre-test probability HF population, the absence of coronary calcification was an effective predictor of the absence of CAD and was thus able to confidently exclude an ischemic etiology. According to these findings, a calcium score threshold of zero can be safely used as a gatekeeper for CTA acquisition in these patients – thus avoiding the small, but non-negligible, risk of complications related to contrast administration and radiation exposure.
Our results are in line with the published literature.18 Abunassar et al. reported that in a population of 153 patients with a history of HF and low LVEF (<50%) all the 13 subjects with ischemic etiology had some degree of coronary calcification as assessed by the calcium score, whereas 30% of the subjects with non-ischemic cardiomyopathy had a Agatston score of zero.18
CAD is believed to be the underlying cause in approximately two-thirds of patients with HF and low LVEF.19,20 The distinction between ischemic and non-ischemic cardiomyopathy and assessment of CAD extent have major clinical implications in patients with dilated cardiomyopathy.21 Clinical data and assessment of pre-test probability based on cardiovascular risk factors have been shown to be unreliable in this differentiation.21,22 Therefore, auxiliary exams are usually necessary. One approach would be the use of functional tests to detect ischemia scar, using nuclear, magnetic resonance or stress echocardiography. Cardiac magnetic resonance (CMR) may be particularly suited for this indication, given its accurate assessment of volumes and biventricular function and its high-resolution ability to detect scarring and to distinguish different patterns of fibrosis according to the underlying etiology. However, the availability of CMR is still limited in some centers and a significant proportion of HF patients are still referred for ICA to assess the coronary tree and to infer the etiology. A recent study demonstrated that nearly two-thirds of patients referred for ICA do not have obstructive CAD (defined as ≥50% stenosis in the left main or ≥70% in any other coronary artery).23 According to this study, ICA may be unnecessary in many patients – and MDCT might be used as an effective non-invasive alternative for the exclusion of CAD.24–26 However, HF patients have distinctive characteristics that may limit the image quality and diagnostic performance of MDCT, particularly reduced apnea capability, higher prevalence of atrial fibrillation and lower cardiac output (which tends to slow the first passage of contrast, leading to contrast dilution and suboptimal vessel opacification). In our study, MDCT image quality was considered diagnostic in the majority of patients and overall performance appears to support its use for exclusion of CAD in this context.
Only a third of patients presented obstructive CAD on CTA, and only 6% had criteria for ICM. This low prevalence of CAD may be explained by the study design, since patients referred for MDCT are usually those with a relatively low probability of CAD. In our study the majority of patients had a low to intermediate pre-test probability, probably reflecting a good clinical selection of candidates for this test, especially suited for the exclusion of CAD.
One particular subgroup of HF patients requiring a focused analysis is the population with AF.27 The reported prevalence of AF in modern heart failure series ranges from 13% to 27%. Moreover, the prevalence of AF in patients with HF increases in parallel with disease severity, ranging from 5% in patients with mild HF to 10%–26% among patients with moderate HF and up to 50% in patients with severe HF.27 In our HF population, with a mean LVEF of 35±7.7%, only 7% of patients presented AF. This low prevalence may be explained, once again, by patient selection. Although AF poses a challenge to MDCT due to typically higher rates and an irregular R-R interval,25 recent studies28,29 have demonstrated that MDCT can still be an option in this context. Also, Marwan et al.30 reported that in 60 patients (15% with unexplained LV dysfunction) with controlled AF (range 32-107 bpm) referred for MDCT for exclusion of CAD the sensitivity, specificity, positive predictive value and negative predictive value were 100%, 85%, 67% and 100%, respectively. Our data, although on only seven AF patients, are consistent with these findings.
Study limitationsWe acknowledge that our study has various limitations. This is a retrospective study, reflecting a single-center experience of patients referred for CTA during diagnostic workup of heart failure. As such, a clear selection bias has to be reported since only patients without known CAD clinically referred for MDCT were included. This resulted in a relatively small population sample with an intermediate to low pre-test probability of CAD and low prevalence of AF and CAD. Therefore, our results cannot be generalized to other populations. Nevertheless, they may be indicative of the value of MDCT in clinically selected patients.
Additionally, the observational and retrospective nature of the study does not allow determination of the sensitivity and specificity of CAC or CTA for the exclusion of an ischemic etiology, since patients did not systematically undergo CTA or ICA.
Another important limitation is the standard for defining CAD and ischemic cardiomyopathy. The use of CTA and ICA, rather than functional assessment, particularly CMR, may limit the actual discrimination of etiologies. Moreover, obstructive CAD as assessed by angiography may be a concomitant disease rather than the etiology of cardiomyopathy. Conversely, myocardial infarction can complicate non-significant coronary stenosis due to spasm or plaque rupture.31
ConclusionIn our intermediate to low pre-test probability HF population, MCDT was able to exclude an ischemic etiology in 73% of cases in a single test. According to our results the Agatston calcium score can serve as a gatekeeper for CTA in patients with HF.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consent.The authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
AuthorshipPAS, NB, NDF, MC, DL and WF performed the CTA. NDF performed the statistical analysis. NB was a major contributor in writing the manuscript. All authors read and approved the final manuscript.
