




A 64-year-old man with a history of saccular aneurysm in the right aortic sinus (RAS) was admitted due to heart failure. Four-dimensional flow magnetic resonance angiography (Figure 1A–C) and transesophageal echocardiography (TEE) (Figure 1D) confirmed a fistula over a funnel structure from the RAS to the right atrium (RA) with left-to-right shunt during the whole cardiac cycle. Right catheterization showed a cardiac output of 15 l (Qp/Qs 2.7) and a mean pulmonary pressure of 42 mmHg. The heart team decided on percutaneous closure.
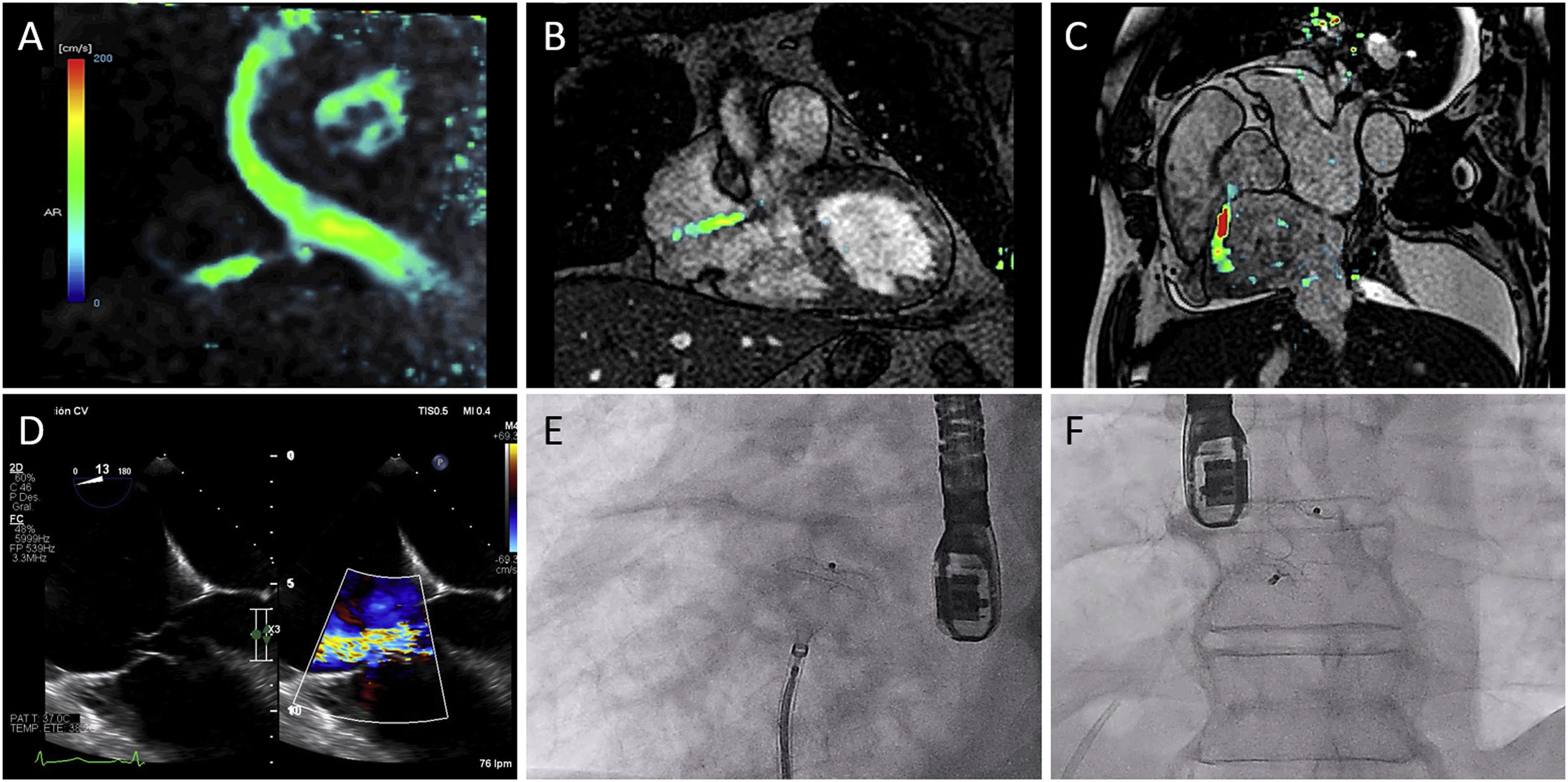
Preprocedural assessment and percutaneous closure. Left-to-right shunt during the entire cardiac cycle between the right aortic sinus and the right atrium can be noted on 4D-flow magnetic resonance angiography (A–C). Transesophageal echocardiography confirmed the shunt and revealed a funnel structure between the inferior aspect of the aortic root and immediately superior to the septal tricuspid leaflet (D). Percutaneous closure was performed employing an Amplatzer Septal Occluder device (Abbot Medical, E and F).
The fistula was crossed with a multipurpose catheter, a hydrophilic guidewire was snared to establish an arteriovenous loop and the delivery system was advanced from the venous aspect. Based on three-dimensional (3D) TEE, we decided to implant an Amplatzer Duct Occluder (ADO), testing with 12- and 16-mm devices without achieving a stable position or reduction of the shunt, in part due to the inability to deploy the device coaxially to the major axis of the tunnel despite the use of a steerable catheter. Finally, a 12-mm Amplatzer Septal Occluder (ASO) (Abbott Medical) was successfully implanted (Figure 1E and F) with minor peridevice leak (Figure 2, 3D-TEE aortic view [A–C] and en-face view [D–F]; before [A and D], and after closure [B and C; E and F]).
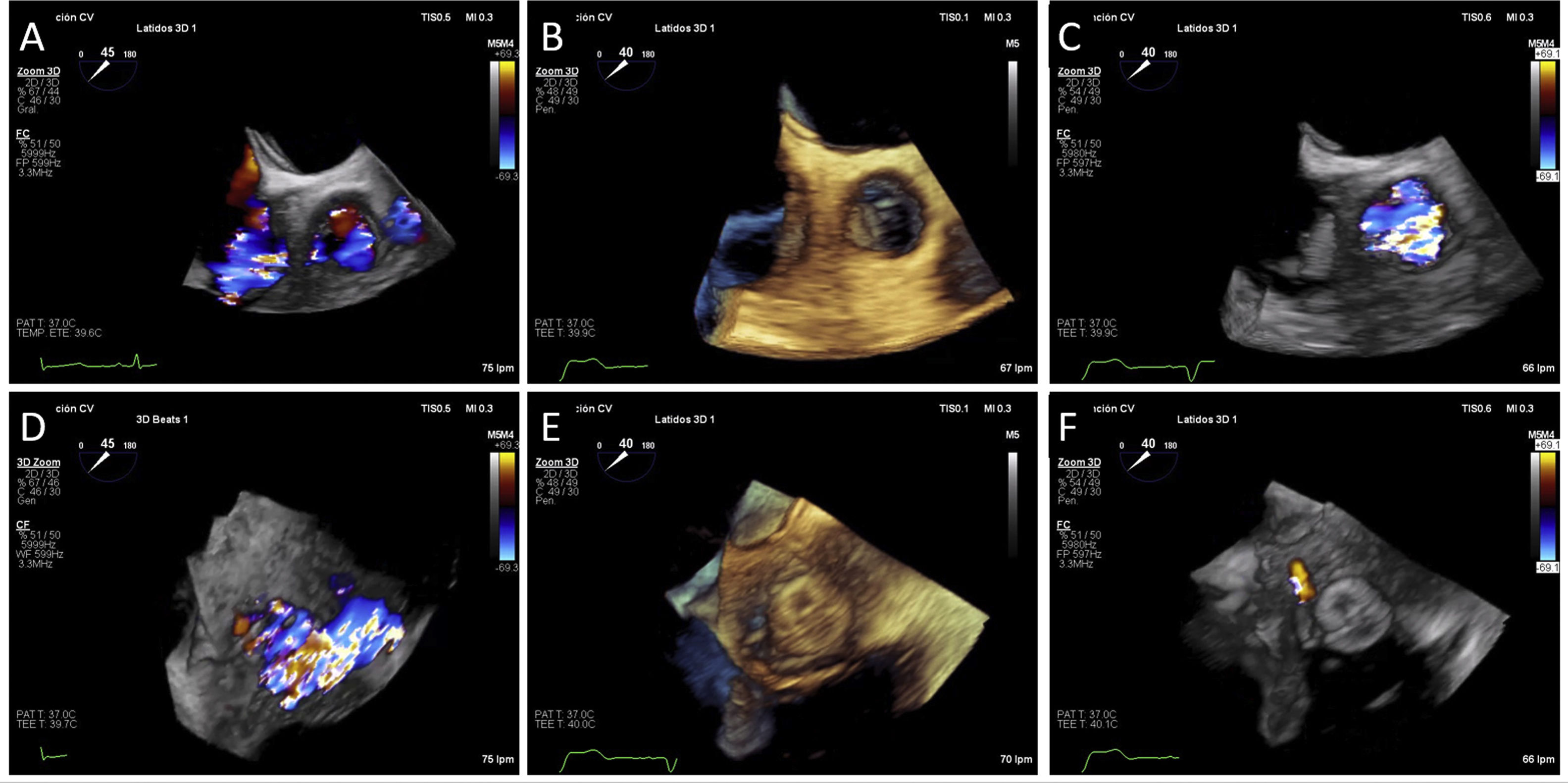
Three-dimensional (3D) transesophageal echocardiographic defect assessment before and after percutaneous closure. Left-to-right shunt assessment before (A and D) and after procedure (B–C and E–F) can be easily compared on the same 3D echocardiography views. A–C: top view from proximal ascending aorta; D–F: en face views of the defect from the right atrium.
Although this type of fistula is widely described, percutaneous closure has been reported almost entirely with ADO devices. To the best of our knowledge, this is the first case of percutaneous closure of an RAS to RA fistula with an ASO device, expanding the portfolio available for this procedure.
FundingDrs. Barreiro-Perez and Cruz-Gonzalez are proctors for Abbott Medical.
Conflicts of interestThe authors have no conflicts of interest to declare.
