







Transposition of the great arteries (TGA) is a rare form of congenital heart disease in which most patients reach adulthood. Right ventricular dysfunction is the most severe residual complication in long-term follow-up, both in patients treated by atrial switch and in those with congenitally corrected TGA. New echocardiographic tools such as longitudinal strain by two-dimensional (2D) speckle tracking may improve assessment of ventricular function in these patients.
Methods and ResultsWe performed a retrospective analysis of echocardiograms in adult patients with TGA (26 patients with dextro-TGA – 15 treated by atrial switch and six by arterial switch – and five with congenitally corrected TGA) and in a control group of 14 healthy individuals. Right ventricular strain was significantly worse (p<0.001), as was the corresponding annular plane systolic excursion (p=0.010) in atrial switch patients, in comparison to arterial switch patients, while no differences were found in left ventricular parameters. In the overall population, systemic right ventricular parameters were significantly less negative than pulmonary right ventricular parameters, and these were less negative than in controls. Left ventricular parameters were similar across groups, except for pulmonary left ventricular strain, which was worse than in controls (p=0.008) as well as pulmonary right ventricular strain.
ConclusionsAssessment of ventricular function in patients with TGA by 2D speckle tracking longitudinal strain is easy and feasible and may be a useful tool for serial follow-up. Of particular note, we found that there is also some degree of ventricular dysfunction even after re-establishment of normal connections.
A Transposição das Grandes Artérias (TGA) é uma cardiopatia congénita rara e a maioria dos doentes atinge a idade adulta. A alteração residual mais grave a longo-prazo é a disfunção ventricular direita (VD), quer em doentes submetidos a switch auricular ou em doentes com TGA congenitamente corrigida (TGAcc). Novas ferramentas ecocardiográficas, como o strain bidimensional por speckle tracking podem facilitar a avaliação da função ventricular nestes doentes.
Métodos e resultadosFoi realizada uma análise retrospetiva de ecocardiograma efetuados em adultos com TGA (26 doentes com dextro-TGA - 15 submetidos a switch auricular e seis a switch arterial – e cinco com TGAcc) e num grupo de controlo composto por 14 indivíduos saudáveis. O strain VD foi significativamente pior (p<0,001) bem como o annular plane systolic excursion correspondente (p=0,010) nos doentes com switch auricular, em comparação com dos doentes com switch arterial, sem diferenças na análise do ventrículo esquerdo. Na população total, os parâmetros do VD sistémico foram significativamente menos negativos do que o VD pulmonar e estes menos negativos comparativamente com o grupo controlo. Os parâmetros ventriculares esquerdos foram semelhantes em todos os grupos, exceto o strain do ventrículo esquerdo pulmonar que é pior comparativamente com o controlo (p=0,008) bem como com o VD pulmonar.
ConclusõesA avaliação da função ventricular em doentes com TGA por strain longitudinal com speckle tracking bidimensional é fácil e pode ser uma ferramenta útil no seguimento destes doentes. De salientar contudo, que verificámos algum grau de disfunção ventricular mesmo após restabelecimento de conexões normais.
annular plane systolic excursion
congenitally corrected transposition of the great arteries
congenital heart disease
dextro-transposition of the great arteries
electrocardiogram
interclass correlation coefficient
magnetic resonance imaging
left ventricular
right ventricular
transposition of the great arteries
In the past 50 years, remarkable advances in the diagnosis and treatment of congenital heart disease (CHD) have resulted in a dramatic improvement in survival of patients with CHD, including in transposition of the great arteries (TGA).1–5 In this severe CHD, the arterial trunks are connected to the morphologically inappropriate ventricles. Presently, most patients reach adulthood both in dextro-transposition of the great arteries (d-TGA) after surgical correction and in congenitally corrected transposition of the great arteries (ccTGA). Until the 1980s, d-TGA patients underwent atrial switch repair with the creation of an atrial baffle to direct venous flow to the contralateral ventricle in the Mustard technique, or by creating a baffle out of autologous tissue in the Senning operation. With these techniques, 30-day perioperative mortality was about 20% but 60% were alive after 30 years of follow-up.2 More recently, the arterial switch operation has become the procedure of choice because it restores normal physiological and anatomic relationships between the arteries and ventricles.
Patients with d-TGA treated by atrial switch and patients with ccTGA have a morphological right ventricle in a subaortic position, which is the main cause of subsequent complications in long-term follow-up.3–6 Echocardiography is the recommended imaging technique for assessment of these patients. However, it is often difficult to assess the right-sided ventricle due to its complex geometry (particularly with qualitative assessment) and changes in ejection fraction or fractional area are late markers of dysfunction. Cardiac magnetic resonance imaging (MRI) is an alternative but limited availability and high cost hinder its use on a routine basis and in serial studies.7 New echocardiographic imaging modalities are now employed in the assessment of ventricular function. Two-dimensional (2D) speckle tracking strain is routinely used to screen for early signs of left and right ventricular dysfunction in adult patients without CHD.8 However, experience with the application of 2D speckle tracking in TGA echocardiography is limited. For this reason, we aimed to test the feasibility of 2D longitudinal strain by speckle tracking for the assessment of ventricular function in adult patients with TGA.
MethodsAll adult patients (aged ≥18 years) with TGA (d-TGA or ccTGA) followed at the outpatient CHD clinic in Santa Marta Hospital (Lisbon, Portugal) and who underwent a routine transthoracic echocardiogram between 2011 and 2016 with adequate digitally stored images were prospectively included in the study. Clinical characteristics were obtained by review of medical files and included age, gender, and type of surgical procedures in cases of d-TGA. A control group of 14 healthy young individuals was also studied for the purpose of comparison.
EchocardiographyA complete standard echocardiographic study was performed including M-mode, 2D and Doppler echocardiography using commercially available systems (Vivid 7™ and Vivid 9™, GE Healthcare). The patient was positioned in left lateral position, and the study was performed with a 3.5 MHz transducer. Annular plane systolic excursion was defined as the maximum distance of systolic movement of the lateral segment of the mitral or tricuspid annulus along its longitudinal plane. For the purpose of strain analysis, images were acquired in apical 4-chamber view, and the transducer settings of the B-mode image were adjusted to achieve a frame rate of at least 55 frames per second (fps) (preferably set at 60-80 fps). The grayscale definition was adjusted as necessary to optimize 2D endocardial and myocardial definitions. Images were digitally stored in cineloop format with three sequential beats and transferred to a workstation for subsequent offline analysis using a customized software package (EchoPAC™, GE Healthcare). The endocardial borders of both ventricles were manually traced and the program automatically generated additional lines near the epicardium. Speckles were then tracked during the cardiac cycle, frame by frame. Whenever necessary, the region of interest was adjusted manually by the operator. Both ventricles were automatically divided into six segments and peak longitudinal strain was averaged from all six segments of the free wall and septum (Figure 1). Peak systolic longitudinal strain was synchronized with the ECG, corresponding to pulmonary or aortic valve closure. Due to the interdependence of the septum being shared between the two ventricles, a separate analysis of the free and lateral wall of each ventricle was also performed. Strain measurements were made by a single operator.
Statistical analysis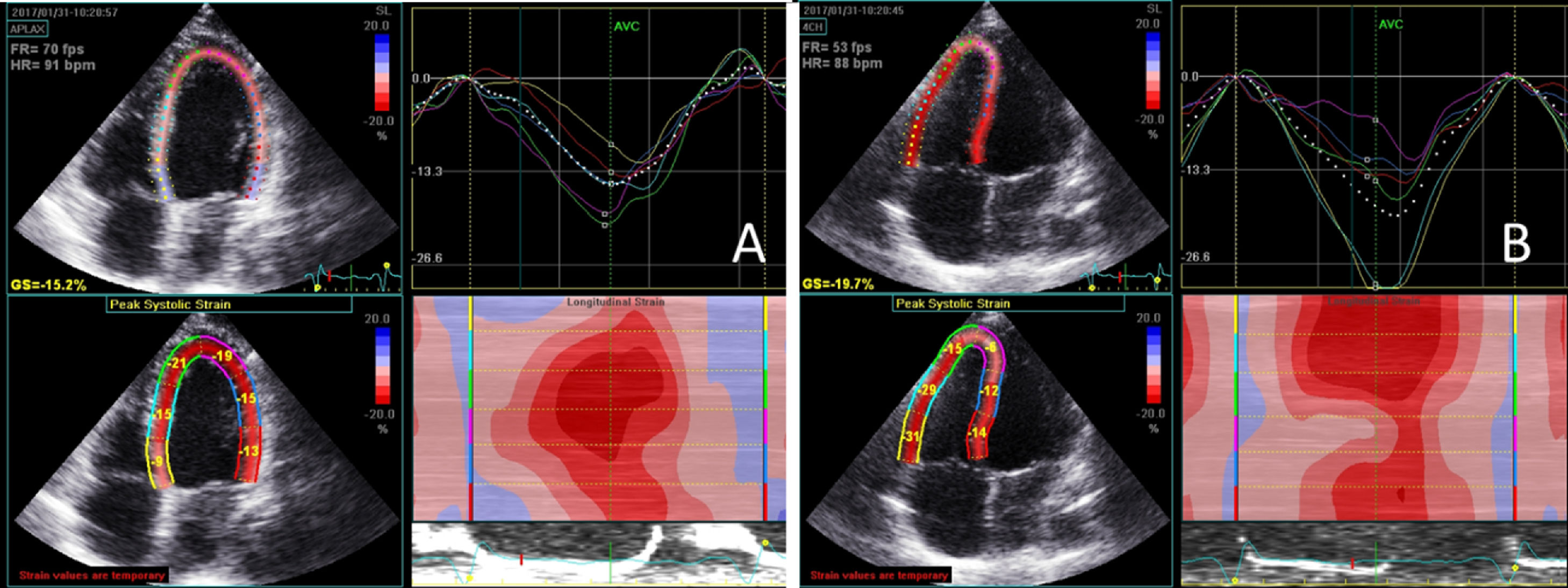
Continuous variables are presented as mean or median, standard deviation or interquartile range (25th percentile-75th percentile), as required. Normality and homogeneity of variance were tested with the Kolmogorov-Smirnov test and Levene's test, respectively. Categorical variables are reported as percentages. Differences between groups for categorical variables were tested with the chi-square test or Fisher's exact test, as appropriate. The Mann-Whitney and Kruskal-Wallis tests were used to compare continuous variables.
To establish and quantify reproducibility of left and right ventricular strain, agreement and intra- and interobserver reproducibility (two operators) were assessed using the interclass correlation coefficient (average measure) and reliability coefficients (Cronbach alpha) with two-way mixed effects models. Mean differences and limits of agreement were also analyzed with Bland-Altman plots. We selected 15 consecutive individuals for reproducibility analysis.
IBM SPSS Statistics software, version 19.0.0.2 (IBM SPSS Inc, Chicago, IL) was used for all statistical analyses. All statistical tests were two-sided with a critical value of 0.05 for statistical significance.
ResultsThe study initially included 40 patients (mean age 32±10 years, 50% male) and 14 healthy individuals (mean age 34±11 years, 50% male). Some patients were excluded due to a poor acoustic window or the presence of additional abnormalities (mainly pulmonary stenosis and ventricular septal defects) that could have biased the results (Figure 2). A final sample of 26 patients was analyzed (21 patients with d-TGA and five with ccTGA; mean age 30±9 years, 54% male).
 ccTGA: congenitally corrected transposition of the great arteries;
ccTGA: congenitally corrected transposition of the great arteries; Systemic right ventricular strain was significantly worse (p<0.001), as was the corresponding annular plane systolic excursion (p=0.010), in atrial switch patients, in comparison to pulmonary right ventricular strain in arterial switch patients (Table 1). In the overall population, systemic right ventricular parameters were significantly worse than pulmonary right ventricular parameters, and these were also worse than in controls, confirming some degree of dysfunction in the pulmonary right ventricle after corrective surgery (Table 2). Left ventricular parameters were similar across all groups, except for pulmonary left ventricular strain, which was worse than in controls (p=0.008). An additional finding was that subpulmonary right ventricular global longitudinal strain was worse than control right ventricular (p<0.05) and similar to left ventricular strain in controls. Global pulmonary left ventricular strain was worse than left and right ventricular strain in controls. However, analysis of free wall strain only showed that this was similar to left ventricular strain in controls.
Comparison of patients with dextro-transposition of the great arteries according to surgery type.
| Systemic RV (atrial switch) (n=15) | Pulmonary RV (arterial switch) (n=6) | p | |
|---|---|---|---|
| Age, years | 30 (25-35) | 24 (22-24) | 0.055 |
| Male gender, % | 62.5 | 36.4 | 0.182 |
| Age at time of surgery, years | 13.4 (5.0 to 20.8) | 0.4 (0.2 to 2.6) | <0.001 |
| Global strain, % | -13.0 (-15.4 to -9.4) | -19.9 (-23.3 to -19.1) | <0.001 |
| Free wall strain, % | -13.3 (- 15.2 to -10.2) | -21.8 (-25.3 to -17.9) | <0.001 |
| APSE, mm | 12.1 (10.9 to 15.8) | 17.7 (14.6 to 19.0) | 0.010 |
Data are presented as median and interquartile range. APSE: annular plane systolic excursion; RV: right ventricle.
Results of echocardiographic study.
| RV comparison | Systemic RV (n=20) | Pulmonary RV (n=6) | Control RV (n=14) | p |
|---|---|---|---|---|
| Age, years | 34 (25-36)a | 23 (20-24) | 33 (26-43) | 0.003 |
| Male gender, % | 65.0a | 0 | 50.0 | 0.020 |
| Global strain, % | -13.0 (-15.2 to -9.4)a,b | -20.9 (-23.6 to -18.9) | -23.4 (-27.8 to -19.8) | <0.001 |
| Free wall strain, % | -13.2 (-14.3 to -10.5)a,b | -21.8 (-25.3 to -17.9)b | -26.8 (-30.4 to -24.1) | <0.001 |
| APSE, mm | 13.0 (11.4 to 15.7)a,b | 17.3 (14.9 to 19.1)b | 21.3 (19.9 to 23.8) | <0.001 |
| LV comparison | Pulmonary LV (n=20) | Systemic LV (n=6) | Control LV (n=14) | p |
|---|---|---|---|---|
| Global strain, % | -16.4 (-20.1 to -11.6)b | -18.2 (-22.7 to -16.1) | -20.0 (-22.0 to -18.5) | 0.028 |
| Free wall strain, % | -22.3 (-24.2 to -8.4) | -18.1 (-22.0 to -14.9) | -22.0 (-24.3 to -20.2) | 0.448 |
| APSE, mm | 17.0 (15.3 to 20.1) | 15.1 (13.2 to 18.1) | 17.5 (15.1 to 19.5) | 0.457 |
Data are presented as median and interquartile range. APSE: annular plane systolic excursion; LV: left ventricle; RV: right ventricle.
Data on reproducibility of results for right and left ventricular strain are presented in Table 3. Reproducibility was excellent in all cases but slightly better for left than for right ventricular strain, particularly for interobserver variability.
Reproducibility of results for right and left ventricular strain.
| ICC (consistency) | ICC (agreement) | Reliability coefficient (Cronbach alpha) | Mean difference (absolute) | Limits of agreement (absolute) | |
|---|---|---|---|---|---|
| RV strain (intraobserver) | 0.982 (0.941-0.991) | 0.981 (0.934-0.992) | 0.989 | -0.42 | ±2.04 |
| RV strain (interobserver) | 0.933 (0.814-0.982) | 0.932 (0.824-0.983) | 0.966 | -0.35 | ±3.84 |
| RA strain (intraobserver) | 0.997 (0.990-0.999) | 0.995 (0.975-0.999) | 0.997 | -0.60 | ±1.66 |
| RA strain (interobserver) | 0.992 (0.978-0.997) | 0.992 (0.976-0.997) | 0.992 | -0.47 | ±2.4 |
ICC: interclass correlation coefficient; RA: right atrial; RV: right ventricular.
The present study demonstrates that assessment of right and left ventricular function by 2D speckle tracking strain is an easy and feasible tool in patients with TGA and may be useful for long-term follow-up. As expected, patients with d-TGA showed the greatest impairment of systemic right ventricular function. However, this imaging technique showed that patients treated by arterial switch also presented some degree of right ventricular dysfunction compared to healthy individuals.
The improvement in survival of patients with d-TGA after surgical correction and the natural history of patients with ccTGA result in the development of late complications, commonly in adulthood, such as heart failure, atrial arrhythmias and sudden cardiac death (particularly in patients with a systemic right ventricle), the incidence of which increases over time. Careful follow-up is necessary and serial imaging is required to analyze changes in systolic function over time.3–6 Right ventricular dysfunction is reported in 48% of patients with d-TGA after atrial switch and symptomatic heart failure in 25% at 15 to 18 years of follow-up, and after 25 years, more than 50% have moderate to severe systemic right ventricular dysfunction.9–12 In the presence of associated cardiac lesions such as ventricular septal defect or pulmonary stenosis it is even more common. In ccTGA, by the age of 45 years, 67% have clinical heart failure in the presence of associated lesions, as opposed to only 15% in the absence of such lesions.3 Early detection of myocardial dysfunction and objective assessment of ventricular function, particularly of the systemic right ventricle, are thus of paramount importance to improve treatment of these patients.
Cardiac MRI remains the gold standard non-invasive technique for structural and functional right and left heart assessment in patients with CHD, including TGA.13 However, its limited availability, high cost and contraindications are important limitations for its application in clinical practice, particularly for serial long-term follow-up of these patients. After atrial switch, echocardiography is recommended for assessment of the systemic right ventricle and integrity of the baffle.7 After arterial switch it is particularly important to screen for coronary stenosis, aortic regurgitation and pulmonary artery stenosis.7 In difficult cases, MRI is recommended to better assess the patency of baffles, baffle leaks, systemic right ventricular function and associated lesions or myocardial fibrosis, particularly when the acoustic window is poor.13 With the introduction of 2D speckle tracking echocardiography, ventricular function can be more easily and thoroughly assessed and dysfunction can be detected at an early stage, but it has not been definitively validated in patients with TGA. With current technology, it can also be assessed online with very short processing times (immediate in most cases).
Previous studies validated annular plane systolic excursion measured by echocardiography compared to ventricular ejection fraction measured by cardiac magnetic resonance imaging, and it is currently used as a measure of ventricular function, particularly for the right ventricle in patients without CHD.13 However, those studies did not take into account the multisegmental nature of contractility. 2D speckle tracking echocardiography is not angle-dependent and is not affected by tethering effects. It can be applied to left and right ventricular functional assessment in patients with CHD, and both right and left ventricular strain are predictors of outcome in other CHD.14–16 It has been tested in patients with pulmonary hypertension, pulmonary embolism, atrial septal defects and tetralogy of Fallot.15–19 Few studies have assessed ventricular function by 2D speckle tracking echocardiography in adult patients with TGA. In these patients systemic right ventricular ejection fraction on MRI correlates well with global longitudinal strain and with fractional area change but not with annular plane systolic excursion, tricuspid s’ with tissue Doppler imaging or systemic right ventricular dP/dT.20
Earlier studies, performed in the late 2000s and early 2010s with older software, showed that global longitudinal strain is significantly reduced in patients with a systemic right ventricle, is related to pulmonary left ventricular function, and predicts adverse clinical outcomes in adults with atrial switch.21,22 Our study, with more recent software, found similar reductions in systemic right ventricular strain, confirming previous data. However, we found that there is also significant change in pulmonary left ventricular strain. A group of young patients (aged <18 years) operated as infants with the Senning procedure were studied by tissue Doppler imaging strain. The authors found that subpulmonary strain values were intermediate between those in the left and right ventricle of normal controls.23 Their explanation for this observation was that the contraction pattern could represent a partial adaptive response to unloading mediated through changes in ventricular geometry (such as a leftward shift of the interventricular septum). In our study, with 2D speckle tracking, pulmonary left ventricular strain was worse than in controls. This is because our patients had corrective surgery at a relatively late age (median 13 years) compared to previous studies, which may have caused residual dysfunction of the pulmonary left ventricle. Our data indicate that this was mainly due to reduced septal strain, because if the septum is excluded from the analysis, strain was similar between pulmonary and control left ventricles.
LimitationsDetermination of right ventricular strain by 2D speckle tracking was performed with non-dedicated software; we used an adaptation of software designed for left ventricular analysis. This could explain the results of our reproducibility analysis. Although the interclass correlation coefficient was excellent for right ventricular strain (better for intraobserver variability), the limits of agreement by Bland-Altman analysis were somewhat wide, particularly for right ventricular strain. Again, the use of non-dedicated software, with frequent manual corrections, may partially explain these results. The other possible explanation is associated with image quality: measurements were more reproducible when image quality was good.
Patients with associated lesions were excluded from the analysis. This is because these lesions, most commonly ventricular septal defect and pulmonary stenosis, are usually associated with a worse outcome, particularly heart failure, and could have confounded our results.
There are also significant variations between different vendors and software.24 For this reason, interpretation of the strain results should take into account the methodology and equipment-specific reference values. It is thus recommended that follow-up assessments should be performed by the same operator and, most importantly, with the same software.
ConclusionsAssessment of right and left ventricular function in patients with TGA by 2D speckle tracking longitudinal strain is feasible and easy and may be useful for serial follow-up. In our population, we confirmed systemic right ventricle dysfunction and also found some degree of ventricular dysfunction in patients with a pulmonary right ventricle after arterial switch in d-TGA as well as in those with a pulmonary left ventricle in atrial switch and ccTGA patients, compared to controls, mainly due to changes in septal deformation. Further long-term prospective multicenter studies are needed for better validation of the clinical impact of this new tool in the follow-up of patients with TGA.
Financial supportThis research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Ethical standardsThe authors assert that all procedures contributing to this work comply with the ethical standards of the 1975 Helsinki Declaration, as revised in 2008. This research does not involve human and/or animal experimentation. All authors contributed to the study design and data acquisition, analysis, and interpretation. The presented manuscript was reviewed and approved by all authors.
Conflicts of interestThe authors have no conflicts of interest to declare.
