



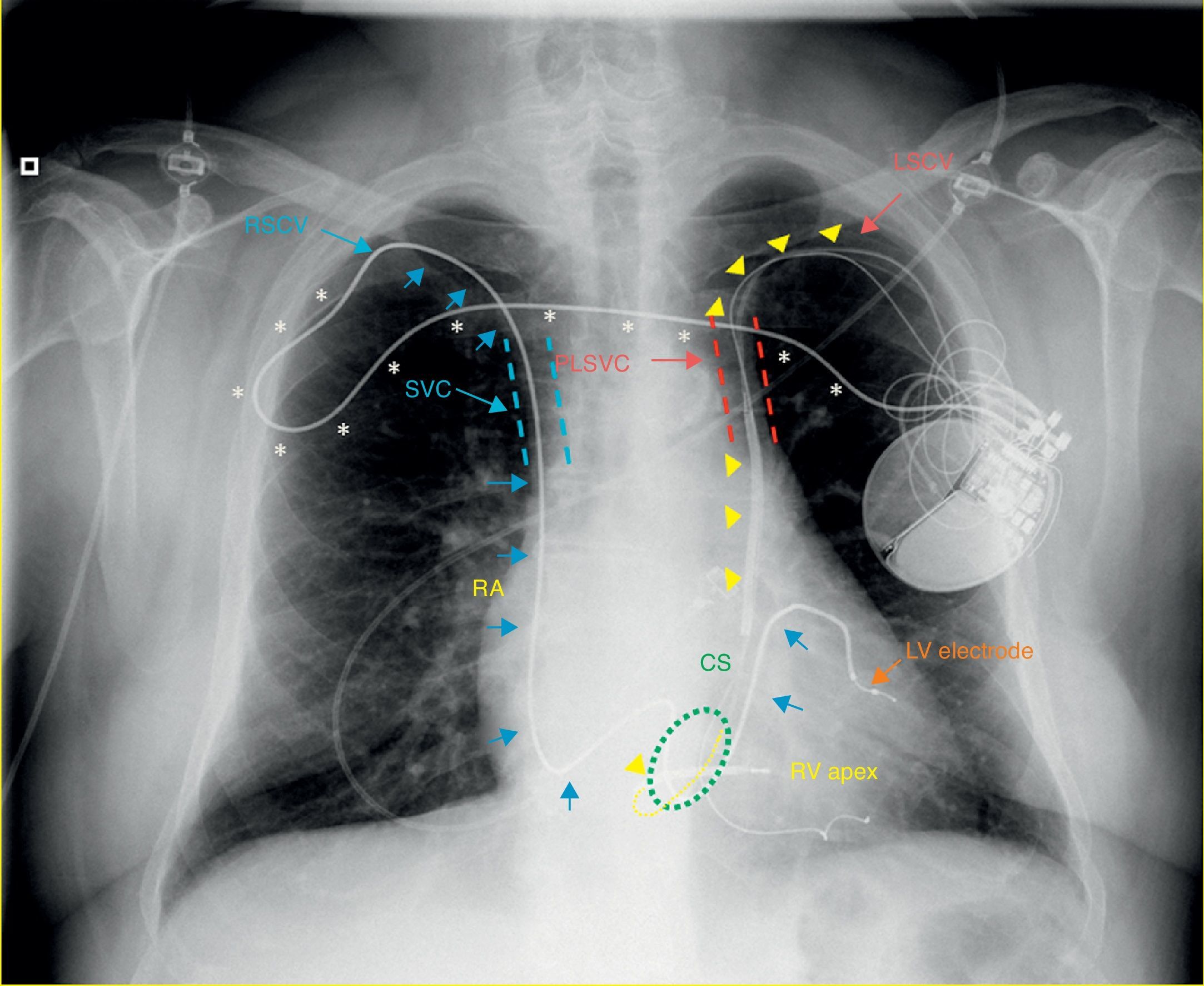
A 64-year-old male with idiopathic cardiomyopathy and atrial fibrillation, previously fitted with a cardioverter-defibrillator (ICD) using a persistent left superior vena cava (PLSVC) for lead placement, was scheduled for upgrade to a cardiac resynchronization therapy-defibrillator due to new-onset left bundle branch block, heart failure and severely depressed left ventricular (LV) ejection fraction. A selective venogram of the coronary sinus from a left-sided approach revealed a sharp angulation of a lateral subsidiary target vein, precluding placement of the LV electrode in an optimal position, and leading to non-controllable diaphragmatic stimulation. A solution was devised by accessing the right subclavian vein and culminating in subcutaneous tunneling of the lead to the contralateral generator pocket. A control chest X-ray with explaining diagram (Figure 1) shows the right ventricular defibrillator lead (yellow arrowheads and dashed yellow line) following a standard left subclavian vein (LSCV) approach but going through a PLSVC draining to the coronary sinus (CS), then entering the right atrium (RA) and crossing the tricuspid valve, with its tip abutting the right ventricular (RV) apex. The LV lead is seen sequentially entering (blue arrows) the right subclavian vein (RSCV), superior vena cava (SVC), RA, CS and lateral vein. Finally, the end of the proximal LV lead (asterisks) is tunneled subcutaneously and connected to the previously placed generator in a left prepectoral position.
Left superior vena cava persistence can occur in up to 0.66% of device candidates and can pose technical challenges during device implantation.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
