

Heart failure (HF) has significant morbidity and mortality, and its prevalence will continue to increase in the future. This unfavorable evolution requires reflection as well as recommendations and decisions based on expert critical and strategic appraisal.
MethodsIn the Acceleration on Heart Failure Empowerment and Awareness – the Portuguese Challenge (ATHENA-PT) study, a range of strategic factors that represent the strengths, weaknesses, threats, and opportunities (SWOT) of HF in Portugal were established. These factors were assessed quantitatively by experts, to create a final SWOT matrix for the management and prevention of HF in Portugal and to outline recommendations.
ResultsFor HF management, the panel emphasized the following strategic recommendations: (i) reimbursement of natriuretic peptides testing in primary healthcare; (ii) reimbursement of Doppler assessment in echocardiographic studies and promotion of detailed information in reports; (iii) intervention to improve the prognosis of patients with HF with preserved ejection fraction; (iv) ensuring effective healthcare transition between hospital and ambulatory units, using checklists/protocols; and (v) reinforcement and commitment to the training of primary health physicians and to the cardiac rehabilitation of patients. For the prevention of HF, the following recommendations/proposals were proposed: (i) campaigns to raise awareness of cardiovascular disease risk factors; (ii) promotion of physical exercise and healthy eating; and (iii) avoidance of therapeutic inertia in the management of risk factors.
ConclusionsThe acknowledgment of various strategic factors and their prioritization by experts made it possible to create and reinforce a range of new strategic recommendations for the management and prevention of HF.
A insuficiência cardíaca (IC) tem morbilidade e mortalidade significativas, prevendo-se no futuro um aumento da sua prevalência. Do reconhecimento dessa evolução desfavorável advém a importância de tecer recomendações e tomar decisões com base em dados valorizados de forma crítica e estratégica.
MétodosNo estudo ATHENA-PT (Acceleration on Heart Failure Empowerment and Awareness – The Portuguese Challenge) foi gerado um conjunto de fatores estratégicos que representam as forças, fragilidades, ameaças e oportunidades (SWOT; Strenghts, Weaknesses, Opportunities, Threats) da IC em Portugal. Esses fatores foram avaliados quantitativamente por peritos, de forma a gerar uma matriz SWOT final para a gestão e prevenção da IC em Portugal e delinear recomendações.
ResultadosPara a gestão da IC, as recomendações incluem: i) comparticipação do doseamento dos pépticos natriuréticos nos cuidados de saúde primários, ii) comparticipação da avaliação com Doppler nos estudos ecocardiográficos e fomento do detalhe nos relatórios, iii) intervenção para melhoria do prognóstico nos doentes com IC com fração de ejeção preservada, iv) promoção da transição fluída de cuidados entre o hospital e o ambulatório utilizando checklists/protocolos e v) reforço e aposta quer na formação dos médicos dos cuidados de saúde primários, quer na reabilitação cardíaca dos doentes. Para a prevenção da IC as recomendações foram no sentido de i) potenciar as campanhas de sensibilização para os fatores de risco cardiovasculares, ii) promover o exercício físico e a alimentação saudável e iii) evitar a inércia terapêutica no controlo dos fatores de risco.
ConclusõesO reconhecimento de vários fatores estratégicos e a sua hierarquização por peritos permitiu gerar e reforçar um conjunto de novas recomendações estratégicas para a gestão e prevenção da IC.
Heart Failure (HF) is a clinical syndrome with rising prevalence,1 especially due to an aging population. The burden of HF is a serious public health issue due to its significant morbidity and mortality. Globally, it is estimated that 64.3 million people live with this condition.2 In Portugal, the EPICA study from the late 1990s estimated a national HF prevalence of 4.36% and expectedly this estimate has increased within older age strata.3 The economic impact of HF in Portugal was evaluated and estimated to be 2.6% of total public health expenditure.4 Considering the aging trends of the population, as well as the weight of the associated comorbidities, HF prevalence and inherent clinical, social and economic costs are expected to increase.4,5
In view of the burden of HF and its epidemiology, it is essential to formulate a comprehensive and critical but also strategic view of this condition to raise awareness among the different stakeholders involved in its future management. The Acceleration on Heart Failure Empowerment and Awareness – the Portuguese Challenge (ATHENA-PT) study aimed to analyze the strategic factors for the management of HF. These factors were evaluated by experts and are proposed to be used to improve the management of this condition in Portugal.
MethodsThe ATHENA-PT study aimed to generate a series of strategic factors attributed values by experts using a methodology adapted from the business administration field: the Strategic Factorial Analysis Summary (SFAS).6
Firstly, an analysis of strategic factors such as strengths, weaknesses, threats, and opportunities (SWOT) was performed through a semi-structured interview. Based on the interview, a SWOT matrix was built for the areas of prevention, diagnosis, treatment, follow-up, rehabilitation, and palliation in HF (considering palliation in the strict sense – symptomatic-based relief in advanced HF).7
In the SWOT analysis, and given that these strategic factors assess an internal domain of HF, known as internal strategic factors, multiple aspects associated with the epidemiology of the syndrome were considered,6 such as the relationship between healthcare professionals and the patient, the processes involved, as well as clinical expertise in HF.7 For the assessment of opportunities and threats, strategic factors related to the external domain (external strategic factors),6 were taken into consideration. These included political, legislative, or financial factors, other competitive aspects in health, and partnerships for the development of knowledge and technology.7 The existence of transitive factors between the internal and external fields enabled us to interpret some data as both weaknesses and threats simultaneously. Therefore, in the same domain, one factor could be considered both as threat and as an opportunity.
Secondly, the matrix was presented as a survey to six medical experts specialized in HF (including cardiologists and internal medicine experts), and to two cardiologists with a strategic and political view in the field of cardiovascular diseases. They were asked to present suggestions of additional factors as well as to assign a relative value (weight – values between 0 and 1) to each strategic factor. In each area assessed, the cumulative value of the number of factors could not exceed 1 (100%). Thus, the global and relative valuation of each strategic factor was expressed as a percentage (%).
The SFAS analysis was performed independently for both HF management and HF prevention to avoid undervaluing HF management factors compared to the prevention field. Management of HF was split into the following domains: diagnosis, treatment, follow-up, rehabilitation and palliation.
The most valued factors were integrated into a final matrix which led to the development of strategic recommendations, by authors, with the purpose of raising the prevention and management standards for HF.
This methodological process took place during the second half of 2021 and ended in the first quarter of 2022.
ResultsAfter the semi-structured interview, 70 strategic factors were identified: 47 related to HF management and 23 related to HF prevention (Figure 1).

Among the 47 factors related to the management of HF (which, as already mentioned, included diagnosis, treatment, follow-up, rehabilitation, and palliation), 28 were internal strategic factors, while 19 were external strategic factors (Supplementary Table 1). Ten internal factors and four external factors were related to the diagnosis of HF; 12 internal factors and 10 external factors were related to the treatment and follow-up of patients; three internal factors and five external factors were related to HF rehabilitation; and three internal factors were related to palliative care.
Among the 23 factors related to HF prevention (Supplementary Table 2), 15 were internal strategic factors, while eight were external strategic factors, all of them being strategic factors for the management of cardiovascular risk factors.
Strategic factors related to heart failure managementFollowing the assignment of factor weighting by the experts, the factor with the highest value within the internal strategic factors was ‘No reimbursement of biomarkers (BNP or NT-proBNP) in primary health care’, with 6.41% (Supplementary Table 3); and within the external strategic factors was related with the possibility of improving the prognosis HF patients with preserved ejection fraction through implementation of innovative medical therapy, with 8.59% (Supplementary Table 4).
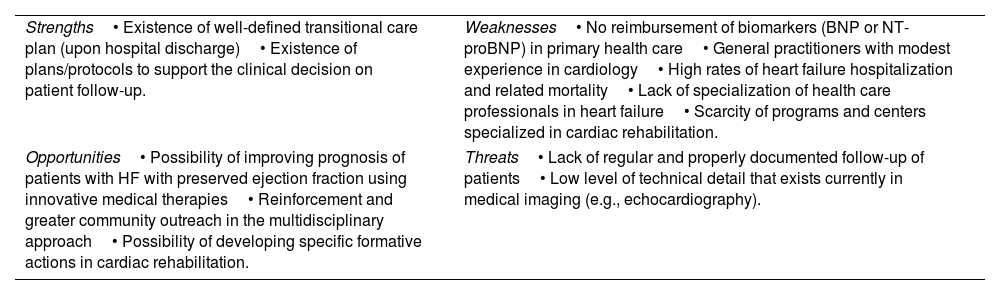
The strategic factors related to HF management are described in Table 1, which represents the reformulation of the SWOT (strengths, weaknesses, opportunities and threats) matrix for the highest valued factors.
Results of the strengths, weaknesses, opportunities and threats analysis with the highest valued factors related to heart failure management.
| Strengths• Existence of well-defined transitional care plan (upon hospital discharge)• Existence of plans/protocols to support the clinical decision on patient follow-up. | Weaknesses• No reimbursement of biomarkers (BNP or NT-proBNP) in primary health care• General practitioners with modest experience in cardiology• High rates of heart failure hospitalization and related mortality• Lack of specialization of health care professionals in heart failure• Scarcity of programs and centers specialized in cardiac rehabilitation. |
| Opportunities• Possibility of improving prognosis of patients with HF with preserved ejection fraction using innovative medical therapies• Reinforcement and greater community outreach in the multidisciplinary approach• Possibility of developing specific formative actions in cardiac rehabilitation. | Threats• Lack of regular and properly documented follow-up of patients• Low level of technical detail that exists currently in medical imaging (e.g., echocardiography). |
The strategic factor with the highest value in the internal strategic factors related with HF prevention was the ‘Low literacy on cardiovascular health’ of the population, with 10.03% (Supplementary Table 5); regarding the external strategic factors, the highest value was for the threat’Suboptimal medication for controlling certain cardiovascular disease risk factors (i.e., arterial hypertension, diabetes mellitus, dyslipidemia)’ with 15.86% (Supplementary Table 6).
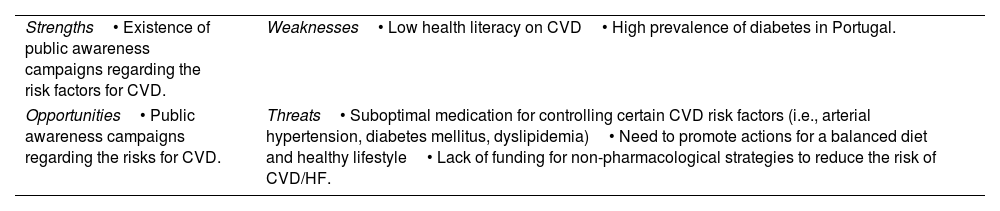
The average relative values are shown in Supplementary Tables 5 and 6, with emphasis on the highest valued strategic factors, which were used to reformulate the SWOT matrix featured in Table 2.
Results of the strengths, weaknesses, opportunities and threats analysis with the highest valued factors related to heart failure prevention.
| Strengths• Existence of public awareness campaigns regarding the risk factors for CVD. | Weaknesses• Low health literacy on CVD• High prevalence of diabetes in Portugal. |
| Opportunities• Public awareness campaigns regarding the risks for CVD. | Threats• Suboptimal medication for controlling certain CVD risk factors (i.e., arterial hypertension, diabetes mellitus, dyslipidemia)• Need to promote actions for a balanced diet and healthy lifestyle• Lack of funding for non-pharmacological strategies to reduce the risk of CVD/HF. |
CVD: cardiovascular disease; HF: heart failure.
In this study we presented the results of a quantitative analysis of strategic factors reflected in the definitive SWOT tables after the consensus obtained within the group of experts.
Management of HFFor the management of HF, diagnostic and therapeutic strategic factors were identified and the most valued are discussed below.
About diagnosis, one of the most emphasized (and valued) aspects was the absence of economic reimbursement by the National Health System for the evaluation of natriuretic peptide (B-type natriuretic peptide (BNP) or NT-proBNP) plasma levels in primary health care, despite the clinical and economic advantages demonstrated in this context.8 It should be noted that the HF diagnosis algorithm of the European Society of Cardiology guidelines suggests that the first-line test to be performed (after an electrocardiogram) should be the quantification of natriuretic peptides.9 Low levels discard HF due to their high negative predictive value10 whereas high levels contribute to an adequate clinical diagnosis in symptomatic patients. The underuse of this test may lead not only to an inadequate management of a disease (due to a presumptive diagnosis of HF that may not be true) but also to a missed opportunity to identify patients with structural and/or functional dysfunction of the heart in need of immediate treatment. Another strategic factor considered negative and associated with diagnostic tests was the frequent scarcity of details included in the technical reports of echocardiograms performed in an outpatient context. Although the elements that must be included in clinical reports need to be standardized,11 it is essential to provide minimum information, such as the left ventricular ejection fraction (using the Simpson method), and the indexed volume of the atria (as well as other important elements), which are relevant for the diagnosis and management of HF patients.11
Another aspect also related to the use of echocardiogram is the lack of reimbursement by the public health service for Doppler assessment in a primary health care setting. Given that this is an essential component of the echocardiographic evaluation (although usually performed informally), it is perceivable that reimbursement would enable a systematic and detailed cardiac evaluation that provides critical and etiological-related information for excluding or supporting an HF diagnosis with reduced, mildly reduced or preserved ejection fraction.
The need to improve the prognosis of patients with HF with preserved ejection fraction was highlighted as an opportunity in the management of HF. This opportunity derives from recently published data on sodium-glucose co-transporter 2 inhibitors. The EMPEROR-Preserved study (using empagliflozin) revealed a decrease in the risk of the composite outcome (of cardiovascular mortality or heart failure hospitalization) comparatively with placebo, essentially at the expense of reduced hospitalizations.12 Recently, dapagliflozin, administered in the DELIVER study, was shown to reduce the risk cardiovascular death or worsening HF in patients with preserved ejection fraction.13 In the PRESERVED-HF study, dapagliflozin was also found to be associated with a significant improvement in symptoms, for example those related to physical limitations and exercise capacity.14 This development is rather insightful considering that, until recently, in HF with preserved ejection fraction there were no pharmacological groups that could robustly modify the prognosis and improve the patient outcomes. This strengthens the need for robust diagnostic tests to identify these patients properly, given that the EMPEROR-Preserved, DELIVER and PRESERVED-HF clinical trials categorized patients according to ejection fraction and natriuretic peptides.12–15 The EMPEROR-Preserved and DELIVER trials included patients with HF with an ejection fraction >40% and NT-proBNP>300 pg/mL (or >900 or 600 pg/mL in the presence of atrial fibrillation in each trial).12,13,15
One of the strategic factors also analyzed by the experts was the existence of well-defined protocols and transition care between hospital and outpatient care. However, non-compliance with these protocols was considered a threat, as well as the lack of a regular follow-up of patients, either during the transition period or after hospitalization. A good example of these transition protocols/guides is a recently published document with a checklist with key elements to be considered in patients with HF before hospital discharge.16 This document compels health professionals to reflect on the adequacy of all aspects of diagnosis, treatment and clinical monitoring and comply with the recommended measures before discharging HF patients.
Also, considering the management of HF, experts highlighted the need for better medical training in the HF field, particularly for primary care/family medicine practitioners to strengthen multidisciplinary networks. Cardiac rehabilitation in HF should also be used more often. Despite the limited number of centers with HF rehabilitation programs, more professionals need to be trained in this area, and more and better rehabilitation programs need to be promoted.
Prevention of heart failureFollowing the SWOT analysis of the strategic factors related to HF, concepts related to awareness campaigns for early diagnosis and cardiovascular risk factors emerged, in addition to the need for greater implementation of non-pharmacological interventions and a relevant concern for the high prevalence of several risk factors, such as diabetes.
For campaigns focused on cardiovascular risk factors, it was concluded that the media (also highlighting the potential of other growing information sources such as social networks) should be used for better dissemination, targeting different age groups. As cardiovascular health literacy in Portugal is low, the experts stressed the need to avoid the trivialization of messages and to find alternative methods and vehicles for transmission.17 For example, the use of social networks, digital influencers, football players etc., to disseminate the existing recommendations effectively.
One of the valued strategic factors concerns the suboptimal medication of cardiovascular risk factors and the concept of therapeutic inertia. In the patients with arterial hypertension and dyslipidemia, for example, therapeutic inertia can be more easily assessed because there are well known individual therapeutic targets. It is estimated that the prevalence of therapeutic inertia is >50%.18,19 The importance of this strategic factor for the long-term improvement of the cardiovascular health of Portuguese individuals is undeniable. This has a relevant potential impact both on the incidence of HF and on its prognosis.
Conclusions and RecommendationsThe evaluation and identification of the highest valued strategic factors by HF the experts, enabled the definition of practical recommendations, including:
- 1.
In the area of HF management
- •
The reimbursement by the national health service of natriuretic peptides in a primary healthcare setting, to add relevant diagnostic information in patients with suspected HF.
- •
The need for greater detail in echocardiogram reports, including the determination of the left ventricular ejection fraction according to the internationally recommended method, as well as the determination of the indexed volumes of cardiac chambers, and the reimbursement of Doppler imaging by the national health service.
- •
Detection of patients with HF with preserved ejection fraction who may benefit from strategies, including pharmacological ones, for the prevention of hospitalization; and efficient organization of healthcare services for this subpopulation of HF patients.
- •
The dissemination and effective use of checklists and protocols in the transition from hospital to outpatient care.
- •
More support for medical training in the HF field, to strengthen and optimize the effectiveness of the network between hospital care and primary healthcare.
- •
The commitment to create new cardiac rehabilitation centers and improve the capacity of current centers, promoting equity in delivery of cardiac rehabilitation in HF.
- •
- 2.
In the area of HF prevention (and overall cardiovascular diseases prevention)
To boost awareness campaigns on the understanding and control of cardiovascular risk factors, using different means and interlocutors. For example, use of social networks, digital influencers, artists, football players etc.
To improve the uptake of regular physical exercise practice and healthy eating by the population.
To consider effective measures to avoid therapeutic inertia in the management of risk factors and to reach the recommended target values. For instance, the inclusion of LDL cholesterol levels in the list of indicators to be evaluated in primary healthcare units, adjusted according to the cardiovascular risk of each patient.
Some of these recommendations were already identified in a paper published in 2017 but have not been addressed,20 which means the messages need to be strengthened for the sake of HF prevention and care in Portugal.
Conflict of interestsISBE (Instituto de Saúde Baseada na Evidência) is a non-profit institution whose purpose is to generate, synthesize, spread and translate into practice the most relevant scientific knowledge and the highest quality in health research. ISBE received an unrestricted grant from Astrazeneca for the planning and conduct of this project, nevertheless the contents of this article of the exclusive responsibility of its authors. DC participated in educational events and/or congresses or conference (which included travel/hospitality) with Bristol-Myers Squibb, Bayer, Boehringer Ingelheim, Daiichi Sankyo, Merck Serono, Ferrer, Pfizer, Novartis, and Roche. DB received fees for lectures, participation in Advisory Boards or Grants for Investigation of AMGEN, Astrazeneca Pharmaceuticals, Boehringer Ingelheim, Linde Health, Merck Portugal, Novartis, Orion, Pfizer, Roche Diagnostics, Servier, and Vifor Pharma. CF fees for lectures, participation in advisory boards or grants for research from AMGEN, Astrazenca, Bayer, Bial, Boehringer Ingelheim, Merck Serono, Novartis, Orion, Pfizer, Roche Diagnostics, Servier and Vifor Pharma. FF received fees for lectures, participation in advisory boards or grants for research from Astrazeneca, Novartis, and Servier. JSC received fees for lectures, participation in advisory boards or grants for research from Abbott, Astrazeneca Pharmaceuticals, Bial, Boehringer Ingelheim, Menarini, Merck Serono, Merck Sharp & Dohme, Novartis, Orion, Pfizer, Sanofi, Servier and Vifor Pharma. BM received fees as speaker and consultancy fees from Astrazeneca, Bayer, Boehringer Ingelheim, Eli Lilly, Servier, Novartis and Vifor Pharma.
The following are the supplementary data to this article:
