






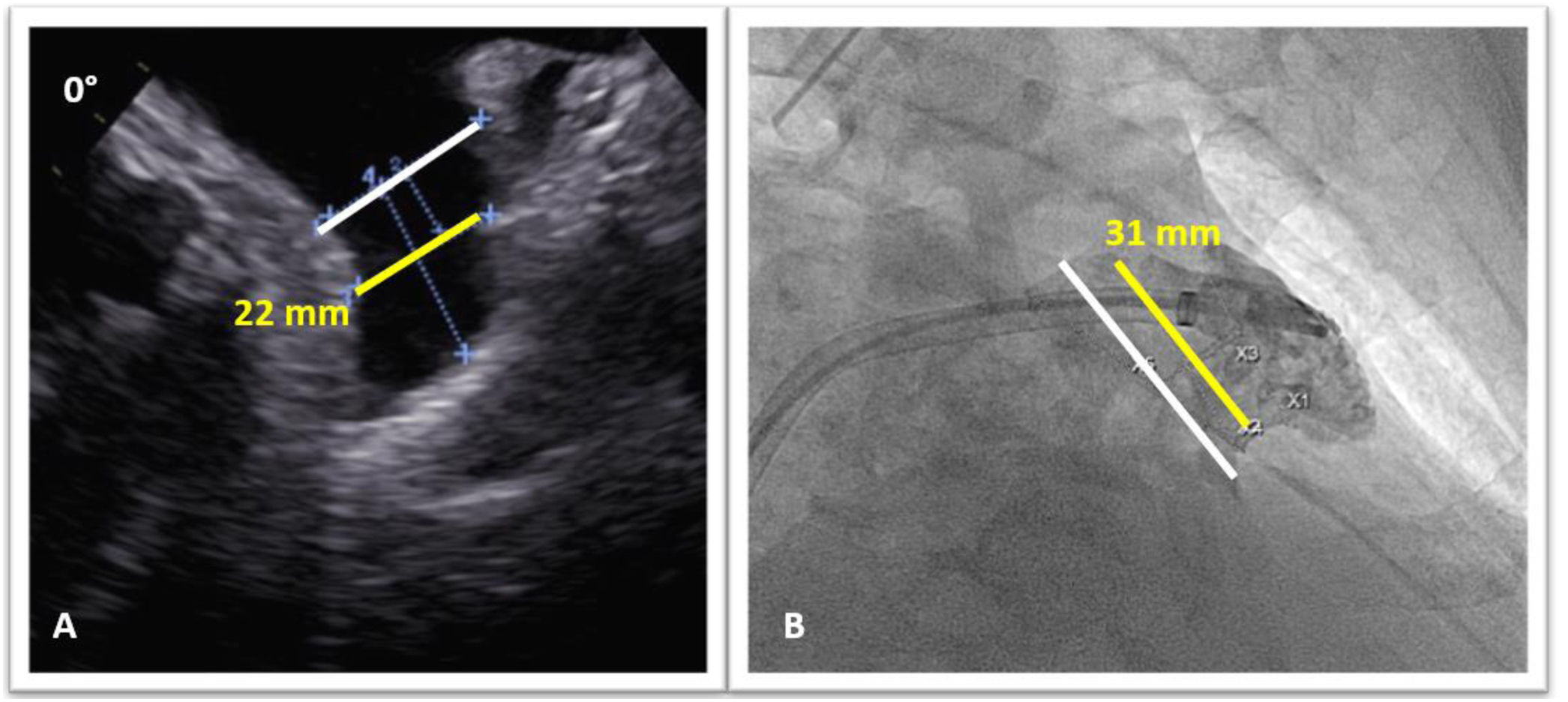
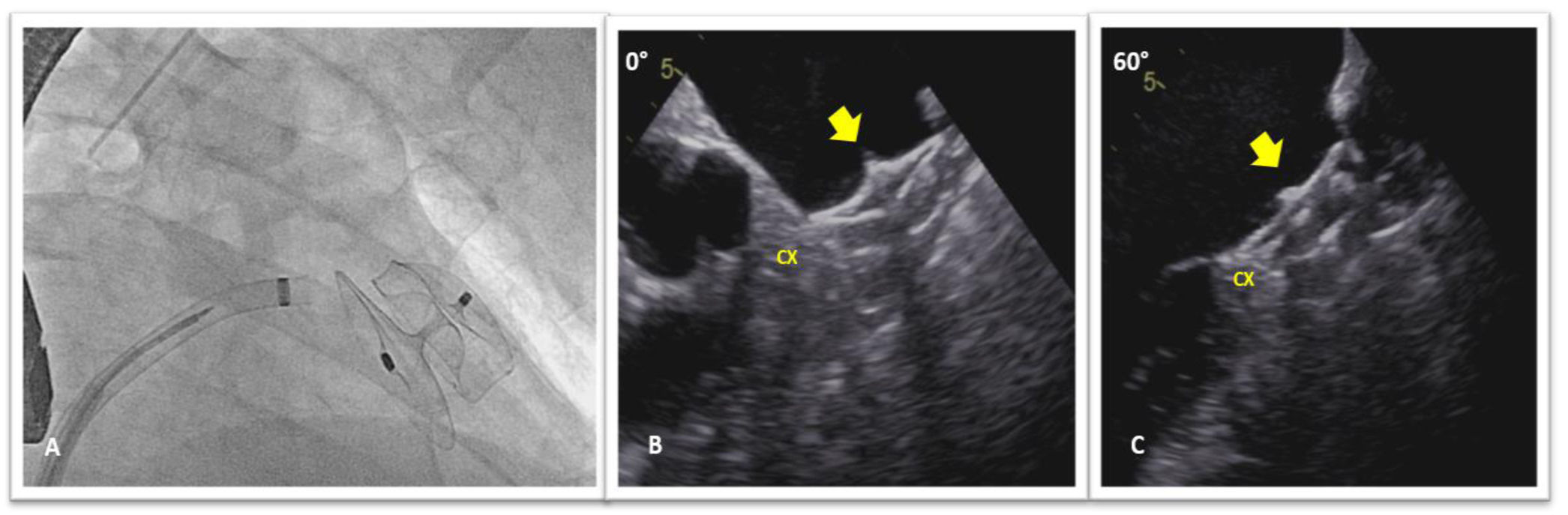
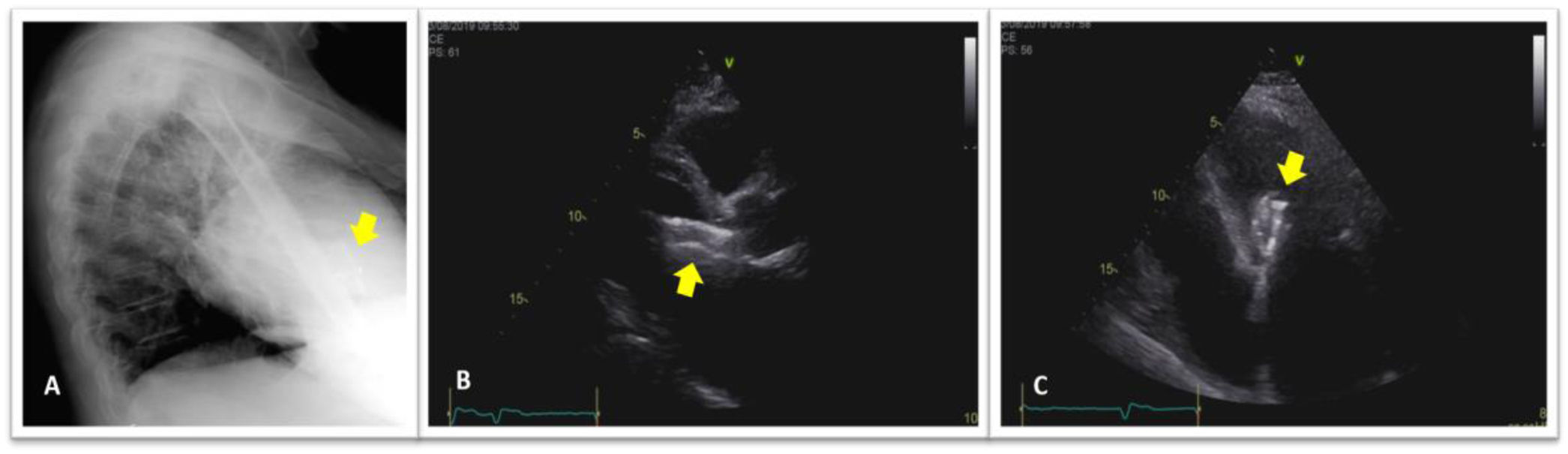
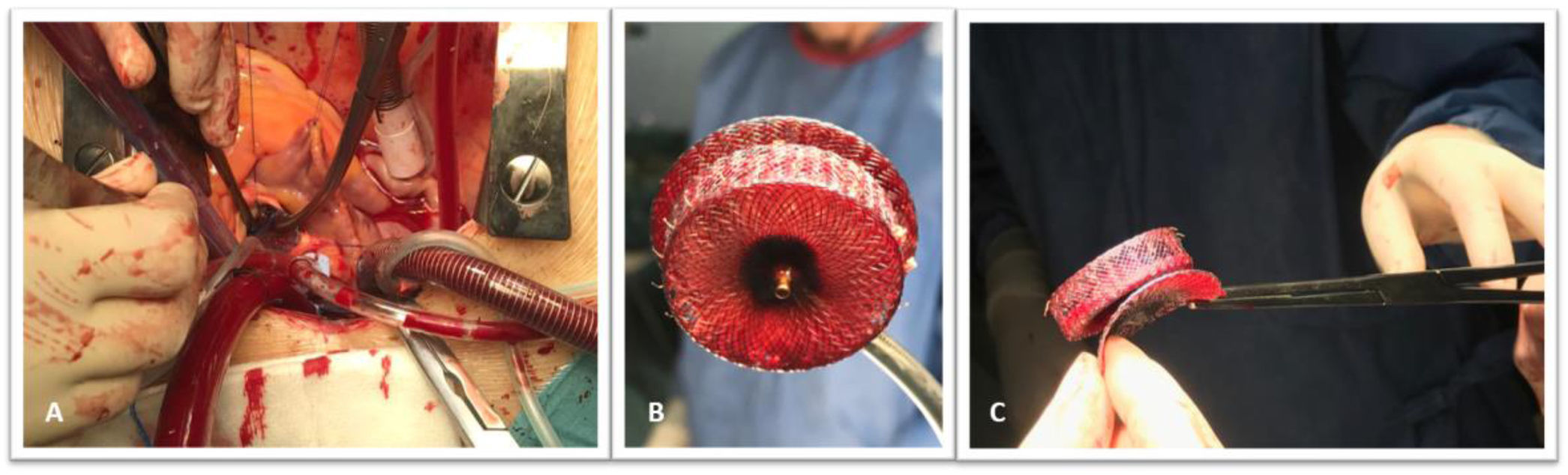
A 68-year old hypertensive man with diabetes and a history of persistent atrial fibrillation and an ischemic cerebral event, was referred for percutaneous left atrial appendage (LAA) closure. He was at high thromboembolic risk based on a CHA2DS2-VASc score of five and oral anticoagulants were contraindicated due to a firearm-related brain injury. A pre-procedure transesophageal echocardiogram (TOE) showed a LAA compatible with percutaneous closure (Figure 1A). It was performed under general anesthesia and with TOE guidance. After transseptal puncture, a windsock-shaped LAA with a landing zone of 31 mm was observed on fluoroscopy (Figure 1B). Based on TOE and fluoroscopy measurements, a 34-mm Amplatzer Amulet device was chosen and deployed in the LAA with a residual leak of 3 mm. Once in place, device stability was confirmed: tire shape of the lobe, concavity of the disk and good separation of the lobe from the disk (Figure 2-A); device lobe was aligned with appendage neck and more than two thirds of the device lobe was located distal to the circumflex artery (Figure 2B and C). The next day, he was asymptomatic and hemodynamically stable, however, a routine chest X-ray (Figure 3A) and transthoracic echocardiogram (Figure 3B and C) showed embolization of the LAA device into the left ventricular outflow tract, without impairment of mitral valve function. Because of the risk of damage to the aortic and mitral valves by the device unfolded anchoring barbs, urgent surgical device removal (Figure 4) and appendage amputation was the first line strategy and the procedure was uneventful.
The authors have no conflicts of interest to declare.
