



A 27-year-old male with known congenitally corrected transposition of the great arteries was referred for further workup due to increasing arrhythmias. Cardiovascular magnetic resonance (CMR) showed situs solitus and atrioventricular (AV) and ventriculoarterial (VA) discordance, with the aorta lying anteriorly and to the right of the pulmonary trunk (Figure 1). An unusual alignment was found, with the right and left ventricular inflow tracts aligned almost perpendicular to one another, precluding imaging all four chambers in one plane. The systemic right ventricle was relatively hypoplastic and lay superior to the subpulmonary left ventricle. The findings were typical of a previously unnoticed criss-cross atrioventricular arrangement. A large nonrestrictive ventricular septal defect and severe pulmonary stenosis were also present; biventricular ejection fraction and indexed volumes were normal and there was no myocardial fibrosis. Antiarrhythmic treatment and an electrophysiological study were proposed.
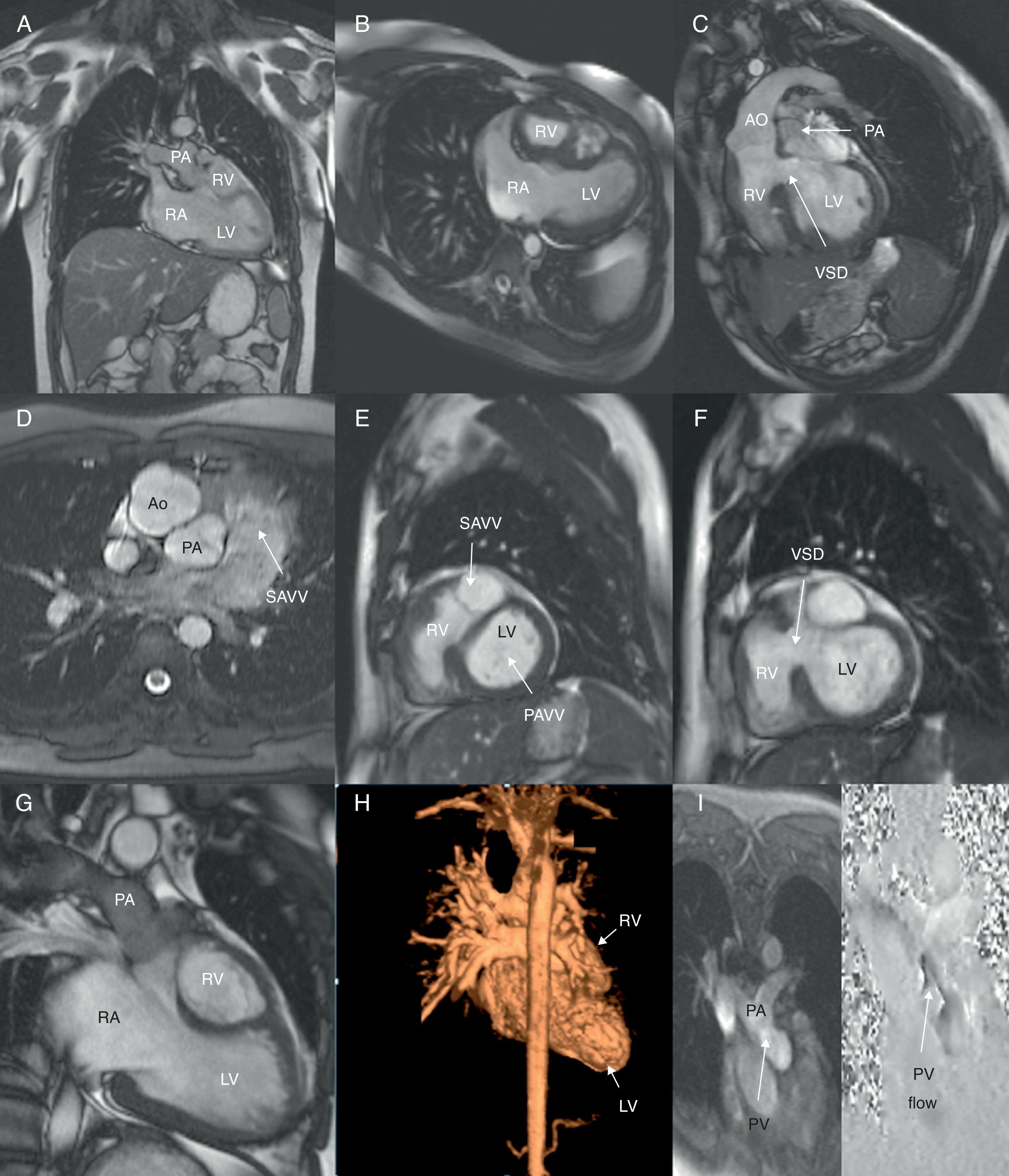
Balanced steady-state free precession (b-SSFP) cine images depicting normal situs (A) and atrioventricular (AV) and ventriculoarterial discordance (B and C, respectively). Note the aorta arising anteriorly and to the right of the pulmonary artery (D). An important clue to the diagnosis of criss-cross heart is the inability to image flow across the two AV valves in the same plane. b-SSFP cine images show this unusual arrangement of the AV valves, perpendicular to one another (E), with the subpulmonary left ventricle (LV) located inferiorly and the smaller systemic right ventricle (RV) superiorly, resulting in a twisted appearance (G); a large (approximately 20 mm) non-restrictive ventricular septal defect is also noted, with bidirectional flow (F). Contrast-enhanced 3D magnetic resonance angiography was performed to help delineate the anatomical relations described above and to assess the great vessels and their branches (H). Phase-contrast velocity mapping of pulmonary stenosis, located at both sub-valvular (from an indented ridge) and valvular level, a common feature of this congenital cardiac anomaly (I). Ao: aorta; LV: left ventricle; PA: pulmonary artery; PAVV: pulmonary AV valve; PV: pulmonary valve; RA: right atrium; RV: right ventricle; SAVV: systemic AV valve; VSD: ventricular septal defect.
Criss-cross heart is a very rare form of congenital heart disease, characterized by this unusual arrangement of cavities, twisted about the long axis, resulting in a superior–inferior relationship of the two ventricles and crossed inflow streams. The exact embryology is unknown. Differential diagnosis includes severe forms of Ebstein's anomaly, double outlet atrium and some forms of atrioventricular valve straddling, which can result in apparently crossed ventricular inflow tracts. Associated malformations determine the outcome.
A segmental approach and multislice imaging are important for determining atrial situs and interpreting AV morphology. CMR, in a single examination, enables unrestricted assessment of this unusual anatomy and the spectrum of associated anomalies for appropriate surgical planning, providing unique data on myocardial scarring.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data and that all the patients included in the study received sufficient information and gave their written informed consent to participate in the study.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interestThe authors have no conflicts of interest to declare.
Dr Francisco Alpendurada, Dr Sonya Babu-Narayan and Dr Philip Kilner are UK Government employees.
