


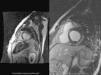


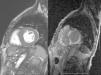



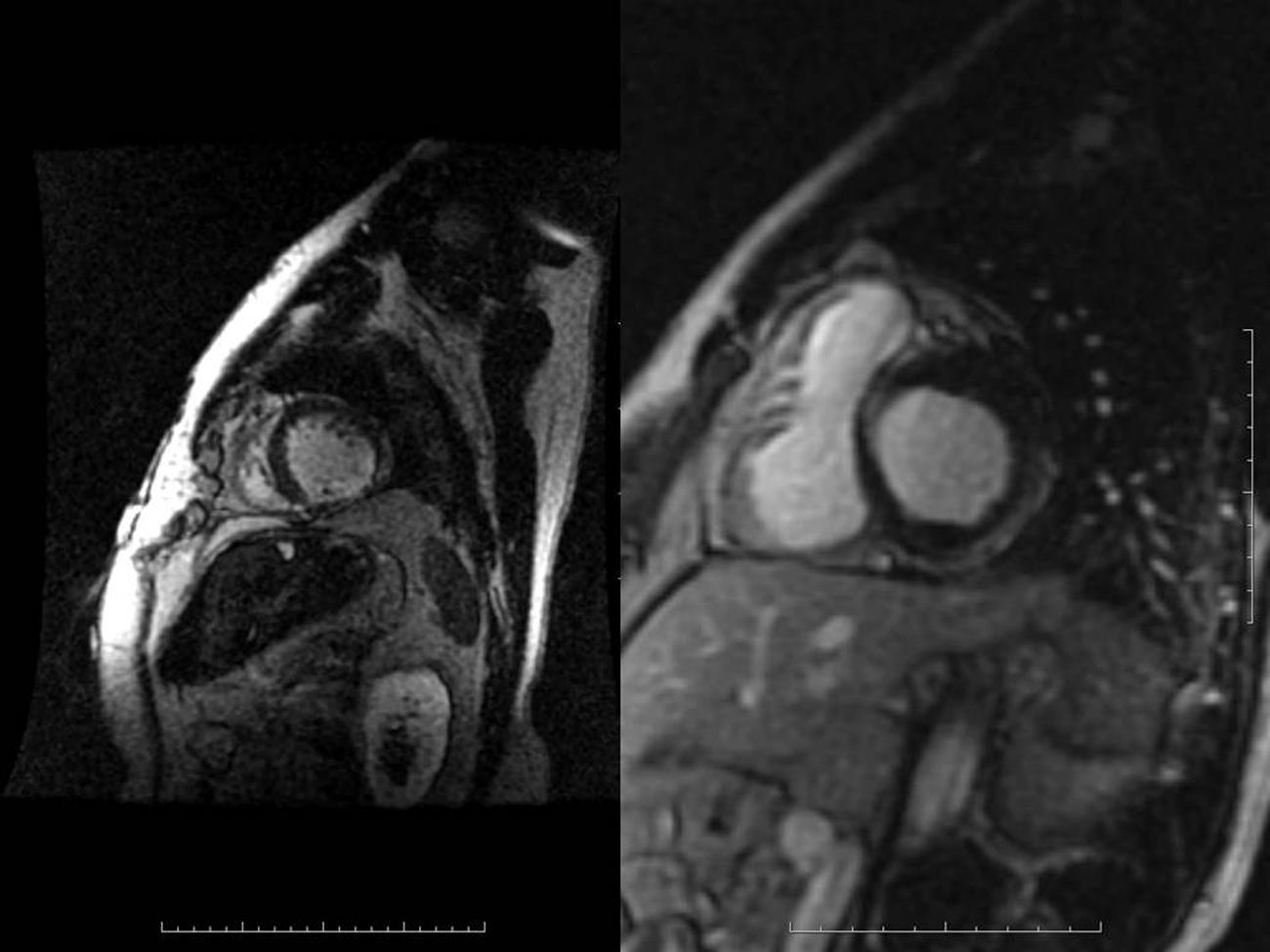
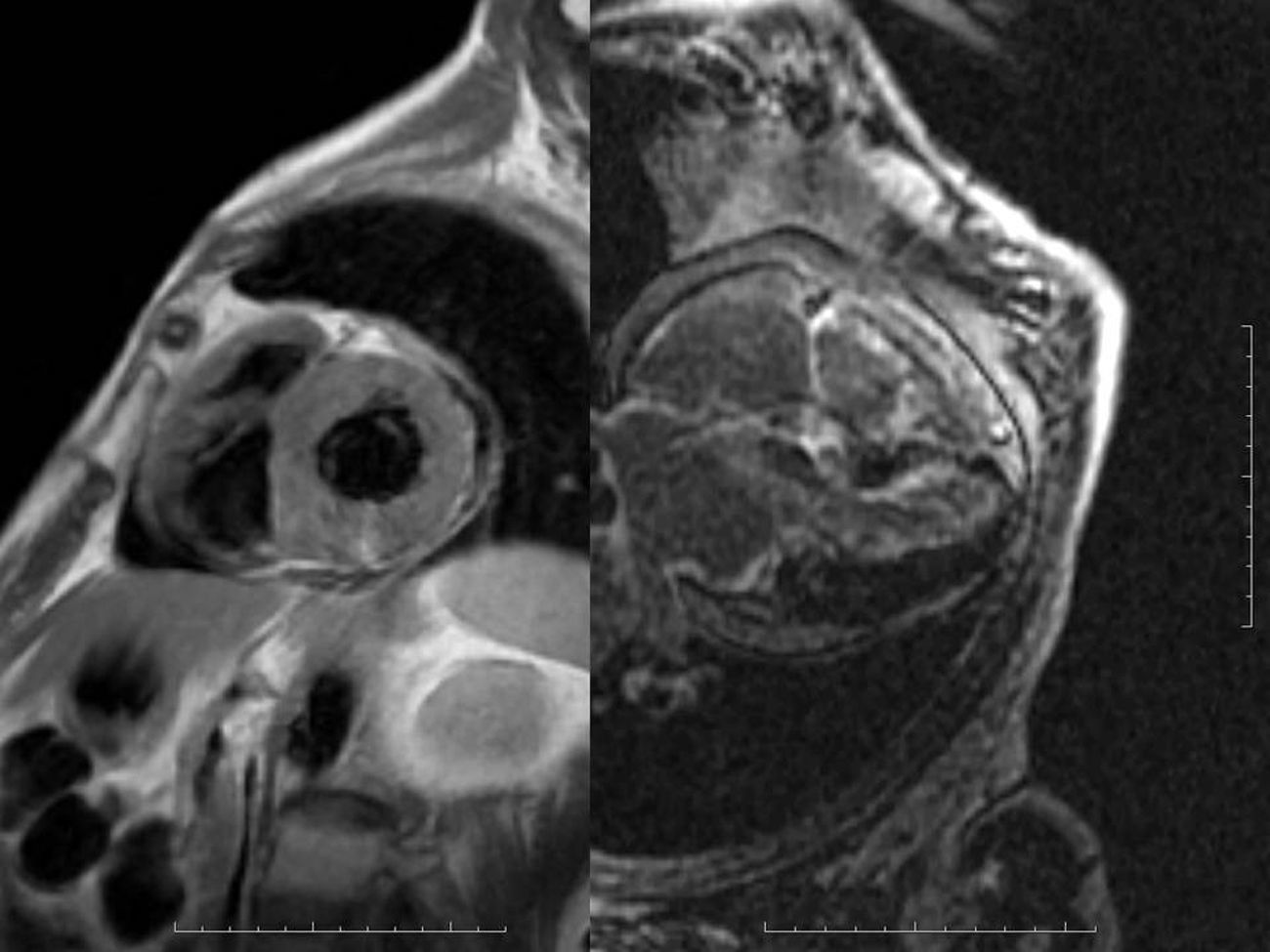
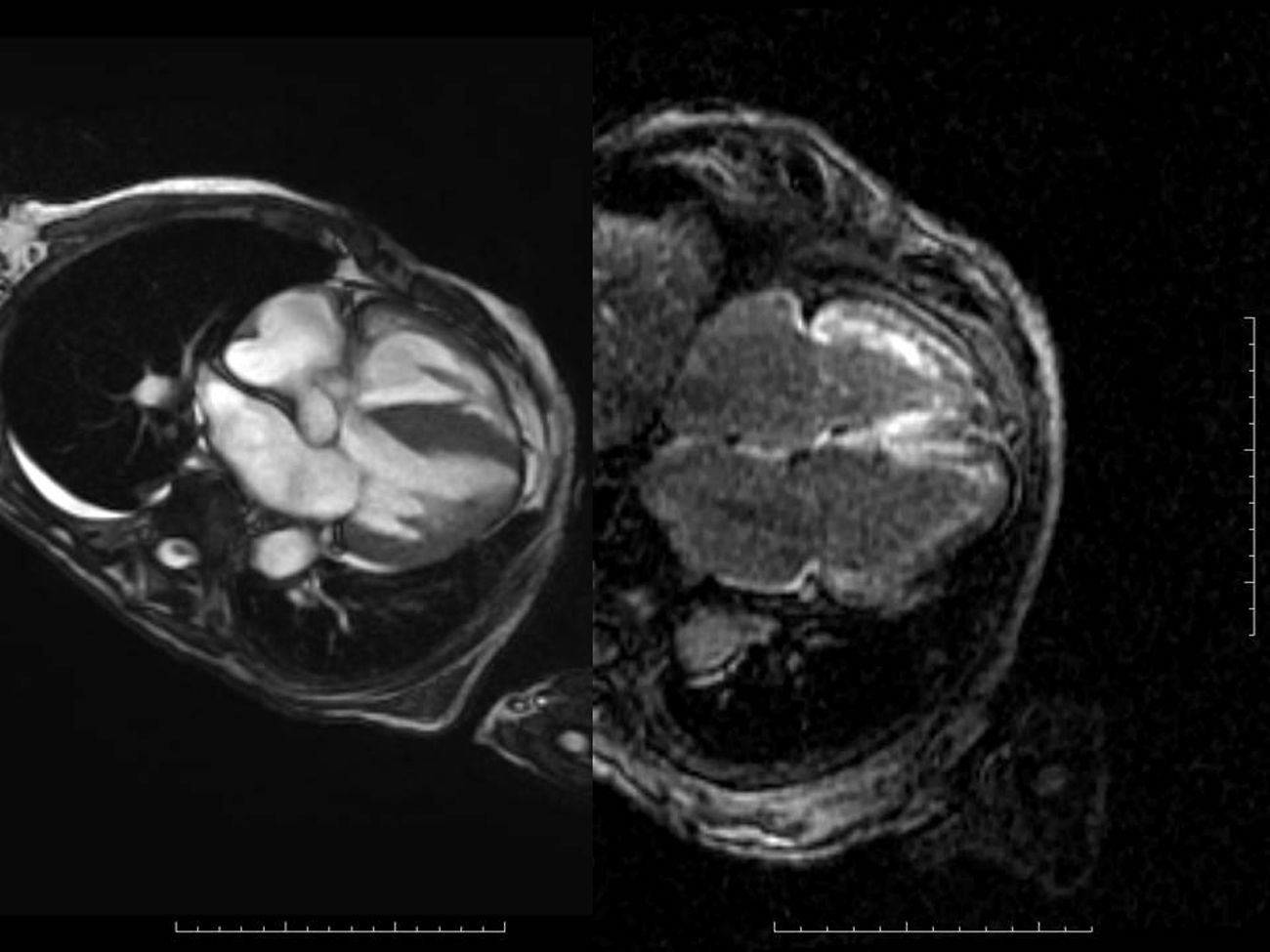
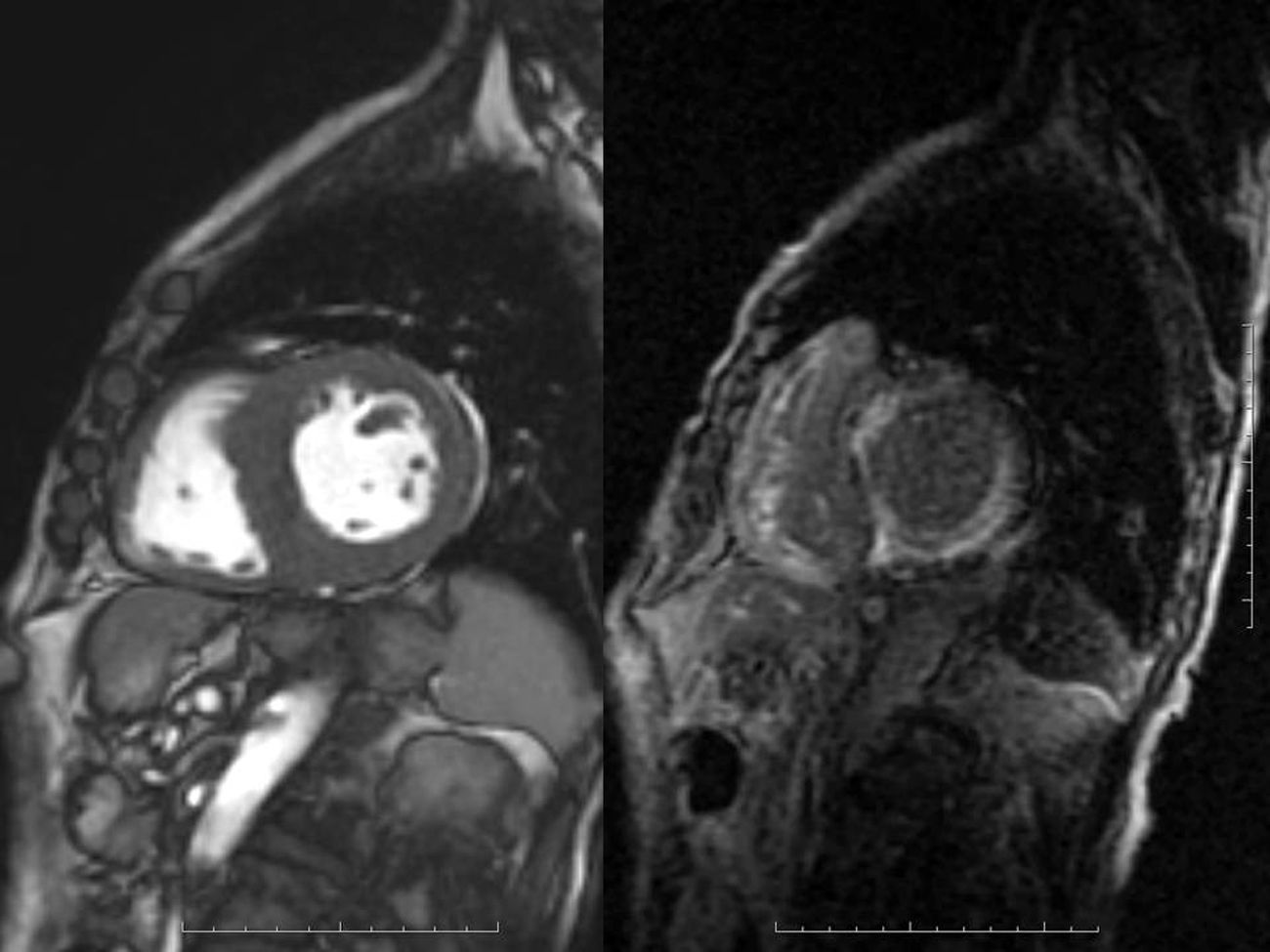
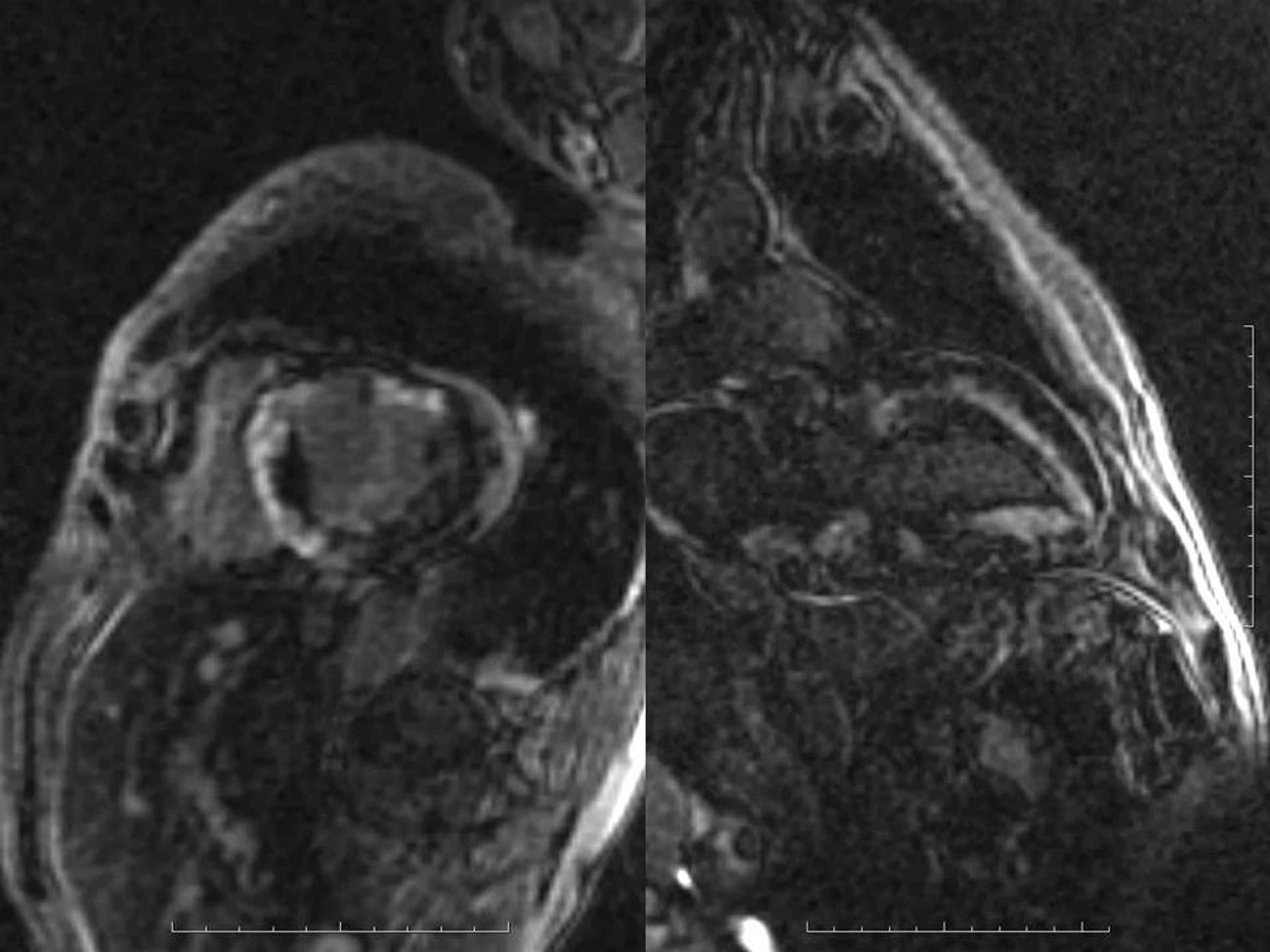
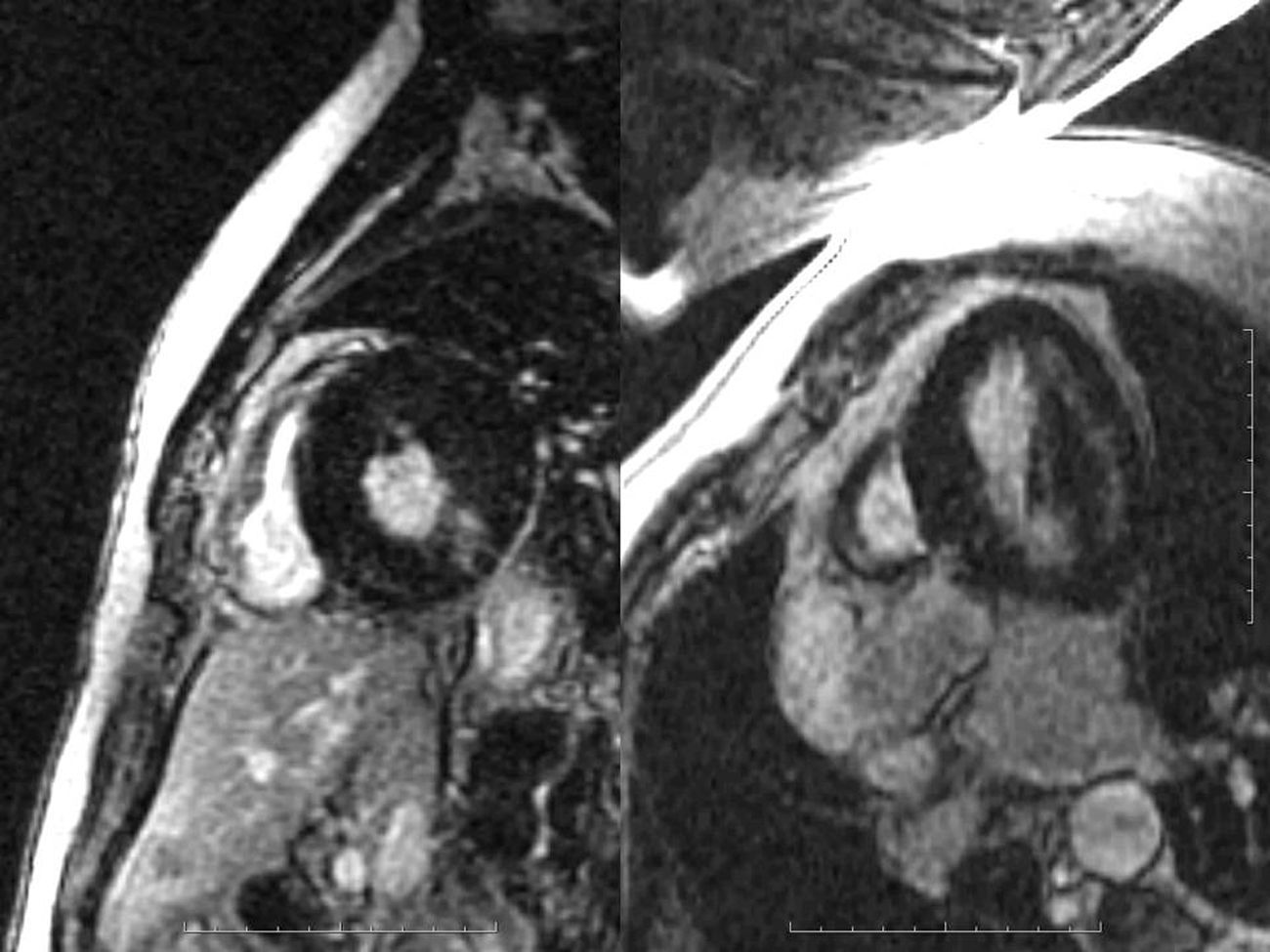
Late gadolinium enhancement (LGE) cardiac magnetic resonance imaging (MRI) is very useful in distinguishing between myocardial infarction, in which the enhancement is typically subendocardial, and myocarditis, in which it is subepicardial (Figure 1). In addition, various patterns have been described with different cardiomyopathies, in some cases enabling a specific diagnosis without invasive workup and risk stratification.1 Cardiac amyloidosis was previously thought to be present only when systemic amyloidosis was patently manifest. This has proved not to be the case, with cardiac MRI detecting increasing numbers of cases in patients with diastolic heart failure in whom cardiac involvement may be the first or sole manifestation. The pattern of LGE commonly found in cardiac amyloidosis is a global subendocardial enhancement with different contrast kinetics, the ventricular cavities showing no signal at all (Figures 2–6) compared to myocarditis and acute myocardial infarction, in which there is an intracavitary gray signal (Figure 1). Of 10 patients referred after echocardiography raised the suspicion of a cardiomyopathy, five were diagnosed with cardiac amyloidosis, two had images not suggestive of amyloidosis and were subsequently found to have Fabry's disease (Figure 7), and the other three probably had concentric left ventricular hypertrophy due to hypertension.

The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
