




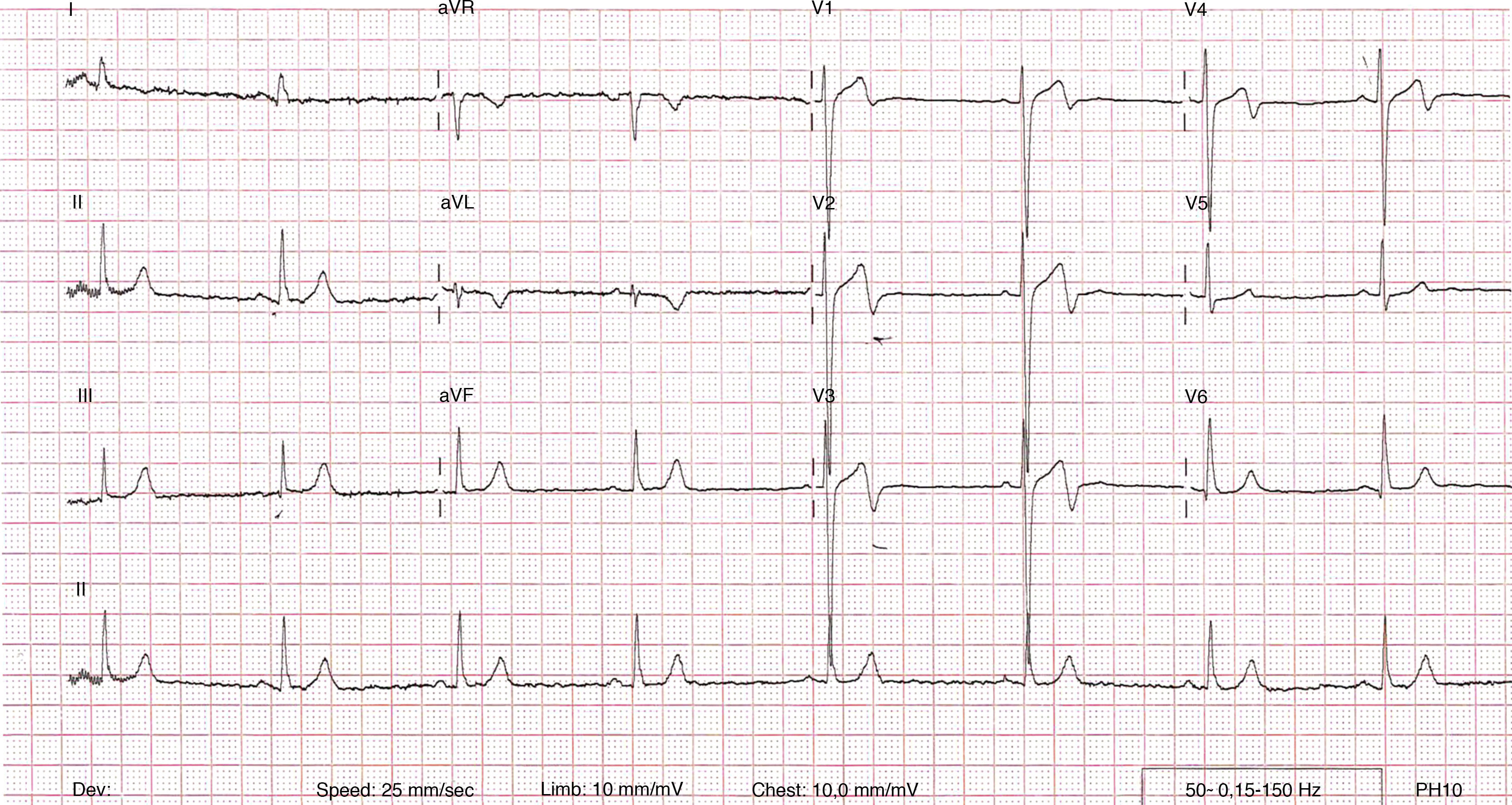
A 28-year-old man presented with a five-hour history of central chest pain and dyspnea. His 12-lead electrocardiogram demonstrated biphasic T waves in leads V1–V4, and T-wave inversion in lead AVL (Figure 1). He was accordingly treated for acute coronary syndrome and referred for coronary computed tomographic angiography (CTA), which showed unobstructed coronary arteries but also an additional vessel that represented a coronary artery fistula (CAF) (Figure 2a–d). In addition there was a bicuspid aortic valve (Figure 2e), concomitant aortopathy (Figure 2f) and a dilated pulmonary artery. The patient underwent surgical ligation of the CAF and was discharged five days later following an uneventful recovery.

(a–c) Three-dimensional volume rendered cardiac computed tomography images showing the relationship of the coronary artery fistula (arrow) to the right ventricular outflow tract, aorta and main pulmonary artery in anterior (a), anterolateral (b) and lateral (c) planes; (d) curved multiplanar reformatted cardiac computed tomographic image showing the course of the coronary artery fistula anterior to the right ventricular outflow tract; (e) multiplanar reformatted cardiac computed tomographic image showing the presence of a non-calcified bicuspid aortic valve; (f) curved multiplanar reformatted cardiac computed tomographic image showing the presence of a concomitant aortopathy. Ao: aorta; LAD: left anterior descending coronary artery; LV: left ventricle; MPA: main pulmonary artery; RVOT: right ventricular outflow tract.
Coronary artery fistulae are usually congenital in origin and account for approximately 0.2–0.4% of all congenital cardiac abnormalities.1 Although commonly asymptomatic, as the fistula progressively enlarges patients may present late in life with dyspnea, fatigue, stroke and endocarditis. Myocardial ischemia may also occur as a result of coronary steal, whereby coronary flow bypasses the myocardial capillary bed in preference for the low-pressure system of the fistula. CAFs in asymptomatic individuals should undergo careful periodic evaluation. In symptomatic individuals, surgical ligation and transcatheter embolization have been shown to be effective therapies.2 The current case firstly demonstrates a rare cause of acute coronary syndrome precipitated by a CAF. Secondly it shows the value of coronary CTA in delineating a CAF and in detecting additional congenital abnormalities. Finally it raises the proposition that CAF may be a coronary anomaly associated with bicuspid aortic valve.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interestThe authors have no conflicts of interest to declare.
