



An asymptomatic five-year-old female was referred due to a heart murmur. Surgical clipping of a patent ductus arteriosus (PDA) had been performed overseas in infancy, but she was subsequently lost to follow-up. The physical exam confirmed a 3/6 continuous murmur in the left subclavicular area and weak left upper extremity pulses. An echocardiogram showed a moderate PDA with continuous left-to-right shunt and mild dilatation of the left heart chambers. Apparently, the ductus arteriosus had not been closed effectively and an elective percutaneous closure was scheduled.
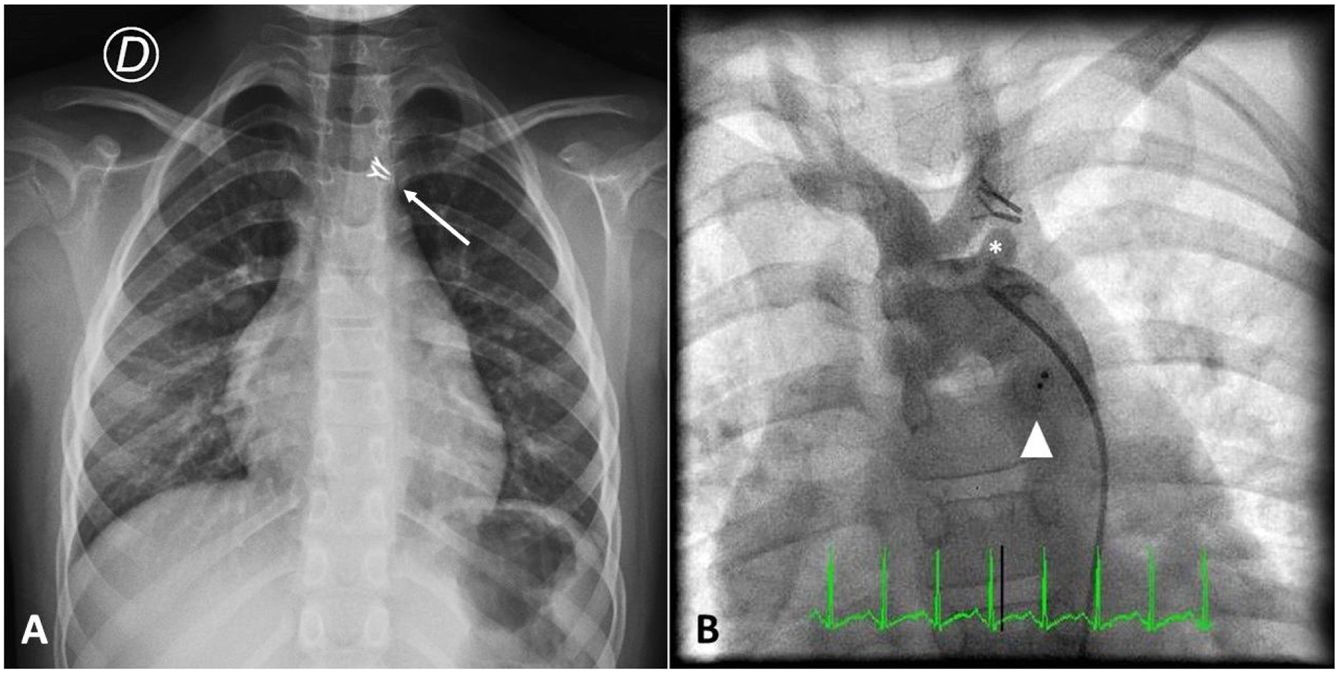
At admission her chest X-ray was normal except for the presence of two surgical clips apical to the cardiac shadow (Figure 1A). Aortic angiography revealed a PDA and, unexpectedly, two vascular clips occluding the left subclavian artery (Figure 1B). Retrograde PDA closure was successfully performed with implantation of an Amplatzer Duct Occluder II. Unfortunately, the clip ligation was considered irreversible. An echocardiogram confirmed ductus closure with no residual leaks. She was discharged home clinically well.
Inadvertent clip placement during surgical PDA closure can cause severe complications including injury to the left recurrent laryngeal or left phrenic nerve1 and occlusion of the left main bronchus2,3 or left pulmonary artery.4 Confirmation of postoperative clip position is therefore imperative.
In our case, X-ray analysis raised suspicions of incorrect ligation due to abnormal apical clip position above the aortic knob. Post-procedure angiography (Figure 1B) clearly confirmed the difference between the closed PDA and the abnormal clip position.
To our knowledge, this is the first report of an iatrogenic left subclavian artery occlusion following surgical PDA closure. Perfusion of the left arm is maintained via the vertebral artery.
Authorship contributionAll authors participated in article preparation. RJP, ML and RA conceived the present report. GN was the patient's pediatric cardiologist. RA carried out the procedure. RJP wrote the paper with input from all authors. ML, GN and RA revised the article. RA and GN were responsible for final approval. All authors approved the final manuscript.
Informed consent was obtained.
FundingNone declared.
Conflicts of interestThe authors have no conflicts of interest to declare.
