
Acute coronary syndrome (ACS) is an important cause of mortality and significant personal and financial costs. Cardiac rehabilitation (CR) programs have shown positive effects in reducing cardiovascular mortality and improving functional capacity. However, adherence is low and appears to be influenced by psychosocial factors, such as patients’ cognitions and emotional state. The objective was to evaluate the efficacy of a brief in-hospital psychological intervention to promote cognitive and emotional adaptation after ACS.
MethodsOne hundred and twenty-one patients with ACS, admitted to a coronary care unit in a central hospital, were randomized to an experimental group (EG, n=65) and a control group (CG, n=56). Portuguese versions of the HADS and BIPQ were used to measure emotional well-being and illness cognitions. Two 1 h 15 min sessions were conducted 2-3 days after hospital admission, and a 20-minute follow-up session took place one month after discharge. Patients were assessed at four different time points: pre-test, post-test, and at 1- and 2-month follow-up.
ResultsThe intervention had significant effects on anxiety, depression and illness cognitions. Anxiety and depression were significantly reduced and illness cognitions improved significantly in the EG compared to the control group. For the EG, these changes were maintained or enhanced at 1- and 2-month follow-up, whereas for the CG there was a deterioration in psychosocial adjustment.
ConclusionsThese results indicate that a brief psychological intervention program delivered during hospitalization for ACS and combined with standard medical care can have positive effects in terms of psychosocial outcomes that have proven impact on cardiac rehabilitation and prognosis.
A síndroma coronária aguda (SCA) é uma importante causa de mortalidade, com custos pessoais e financeiros consideráveis. Os programas de reabilitação cardíaca têm benefícios na redução da mortalidade e melhoria da capacidade funcional. Contudo, a adesão é baixa e depende de fatores como o estado emocional e as representações de doença. Neste trabalho, avaliou-se a eficácia de um programa de intervenção psicológica breve na fase I da reabilitação cardíaca da SCA.
Material e métodosCento e vinte e um doentes com SCA, admitidos na unidade coronária de um hospital central, foram aleatorizados num grupo experimental (GE) (n= 65) e num grupo de controlo (GC) (n=56). Foram utilizadas versões portuguesas da HADS e IPQ-B para avaliar a adaptação emocional e as representações de doença. Foram efetuadas duas sessões de 1 h15 min, 2-3 dias após a admissão hospitalar, e uma avaliação de follow-up um mês após a alta hospitalar de 20 min. Os doentes foram avaliados em quatro momentos: pré-teste, pós-teste, um e dois meses follow-up.
ResultadosOs resultados demonstraram um efeito positivo e significativo da intervenção. A ansiedade e depressão evidenciaram uma redução significativa e as representações de doença melhoraram significativamente no GE, comparativamente ao GC. No GE estas alterações mantiveram-se ou aumentaram no follow-up de um e dois meses, enquanto no GC houve uma deterioração no ajustamento psicológico.
ConclusõesA intervenção psicológica breve durante a hospitalização por SCA, aliada ao tratamento médico convencional, pode ter efeitos positivos em termos de adaptação psicossocial, cujo impacto está amplamente demonstrado na reabilitação cardíaca e no prognóstico clínico.
Cardiovascular disease (CVD), particularly acute coronary syndrome (ACS), is an important cause of mortality in developed countries and is responsible for a large number of hospital admissions, as well as for significant personal and financial costs.1 Cardiac rehabilitation (CR) programs reduce cardiovascular mortality, all-cause mortality and non-fatal ACS and facilitate physical and psychological recovery following acute events.2–5 Furthermore, CR significantly reduces the associated burden on healthcare by maximizing physical, psychological and social functioning and promoting behaviors that reduce or prevent the recurrence of acute events.5,6 Despite the plentiful evidence supporting the effectiveness of CR, studies show that there is low adherence to these programs,7–9 with participation rates varying from 21 to 75%.6,10,11 Two surveys in European countries concluded that less than half of eligible patients participate in CR programs in most countries.10,11
The negative impact of ACS on patients’ psychological functioning has been linked to a lower adherence to therapy and consequently to greater cardiac vulnerability, constituting a higher risk for the recurrence of an acute event.12,13 Multidisciplinary programs that include a psychological component appear to be highly effective and have shown significant benefits in post-ACS morbidity and mortality.14–16 Various clinical trials assessing the effectiveness of such programs have supported the provision of biopsychosocial care in hospital-based cardiac rehabilitation.17,18
In Portugal, research in this area is still scarce and clinical trials on psychological intervention in CR are practically non-existent. This study aims to assess the effectiveness of a brief multidisciplinary psycho-educational intervention in hospitalized ACS patients targeting various psychosocial and behavioral outcomes.
MethodsParticipants and designThe sample consisted of 121 patients (36 females and 84 males), diagnosed with ACS and admitted to the coronary care unit of a central hospital in Portugal. Mean age was 63.78 years (standard deviation 12.48) and 48% of the sample had six or more years of education. Informed consent was obtained from all participants included in the study, which was approved by the ethics committee.
Patients were randomized to an experimental group (EG, n=65) and a control group (CG, n=56), at the time of admission to the coronary care unit, using consecutive weekly randomization (e.g. week 1 for EG and week 2 for CG). Patients were assessed at four time points: hospital admission – pre-test (T1), hospital discharge – post-test (T2), 1-month follow-up (T3) and 2-month follow-up (T4).
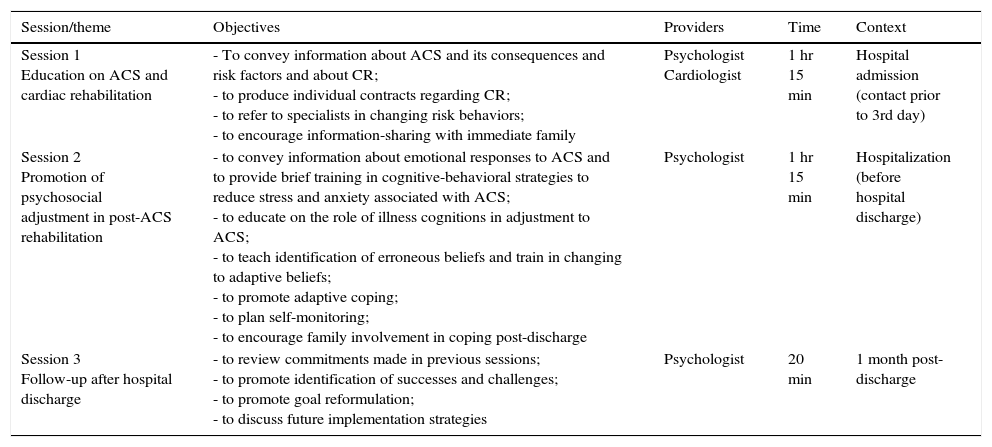
Patients in the EG underwent an intervention within 2-3 days of hospital admission, consisting of two sessions (1 hr 15 min each) and a follow-up session (20 min) at one month after hospital discharge (Table 1). The intervention modality was in group format (mean of six participants per group) and included: (a) health education about ACS and cardiac rehabilitation (session 1) and (b) promotion of psychosocial adjustment in post-ACS rehabilitation (session 2). During the first session information regarding ACS and CR was presented, and patients produced individual contracts regarding the CR program and were encouraged to share information with family members. They were also referred to a specialist in changing risk behaviors. The second session, which took place before hospital discharge, focused on the emotional response to ACS and the importance of illness cognitions in adjustment and adaptive coping. Patients were taught cognitive-behavioral strategies to reduce stress and anxiety, how to identify erroneous beliefs and change them into adaptive ones, and self-monitoring; family involvement was once more encouraged. Session 3 was a follow-up session one month post-discharge and focused on reviewing previous commitments, identifying successes and challenges, promoting goal reformulation and discussing future implementation strategies.
Structure of the brief psychosocial intervention program in post-acute coronary syndrome rehabilitation.
| Session/theme | Objectives | Providers | Time | Context |
|---|---|---|---|---|
| Session 1 Education on ACS and cardiac rehabilitation | - To convey information about ACS and its consequences and risk factors and about CR; - to produce individual contracts regarding CR; - to refer to specialists in changing risk behaviors; - to encourage information-sharing with immediate family | Psychologist Cardiologist | 1 hr 15 min | Hospital admission (contact prior to 3rd day) |
| Session 2 Promotion of psychosocial adjustment in post-ACS rehabilitation | - to convey information about emotional responses to ACS and to provide brief training in cognitive-behavioral strategies to reduce stress and anxiety associated with ACS; - to educate on the role of illness cognitions in adjustment to ACS; - to teach identification of erroneous beliefs and train in changing to adaptive beliefs; - to promote adaptive coping; - to plan self-monitoring; - to encourage family involvement in coping post-discharge | Psychologist | 1 hr 15 min | Hospitalization (before hospital discharge) |
| Session 3 Follow-up after hospital discharge | - to review commitments made in previous sessions; - to promote identification of successes and challenges; - to promote goal reformulation; - to discuss future implementation strategies | Psychologist | 20 min | 1 month post-discharge |
ACS: acute coronary syndrome; CR: cardiac rehabilitation.
The following two hypotheses were tested: (1) we expected that the EG (psychosocial intervention) would present significantly better outcomes at post-test than the CG in terms of anxiety, depression and illness cognitions; (2) we also expected that these gains would be maintained over 1- and 2-month follow-up.
InstrumentsThe instruments used were the Portuguese versions of the Hospital Anxiety and Depression Scale (HADS) and the Brief Illness Perception Questionnaire (BIPQ). The Portuguese version of the HADS,19 which has similar psychometric properties to the original scale, consists of two subscales measuring levels of anxiety and depression. The Portuguese version of the BIPQ,20 which has similar psychometric properties to the original scale, consists of nine items that assess cognitive and emotional representations of illness: consequences, timeline, personal control, treatment control, identity, concern, and emotions, plus one assessing comprehensibility and an open question about the three most important causes of their illness.
Statistical analysisStatistical analyses were conducted using the Statistical Package for the Social Sciences (SPSS), version 19.0. Univariate and multivariate repeated measures statistical procedures were used to test hypotheses. Age and pre-test values of the outcome variables were entered as covariates. Equivalence of the experimental and control groups at pre-test in terms of demographic and psychosocial variables was established using group comparison statistics (the chi-square test for nominal variables and the t test for continuous variables).
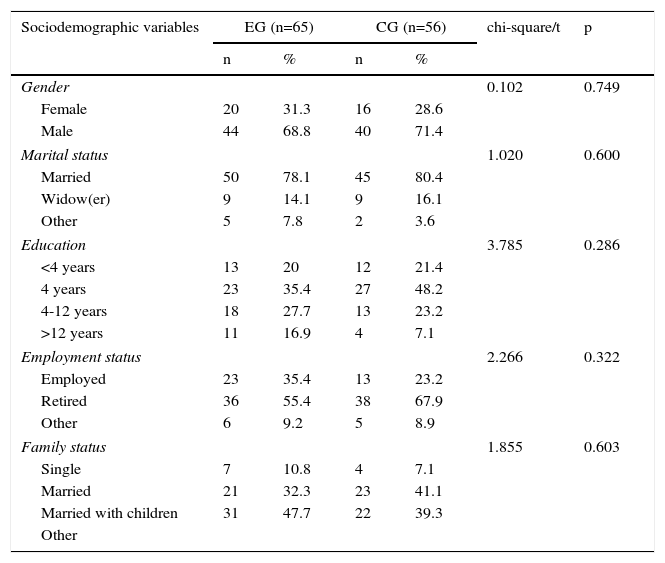
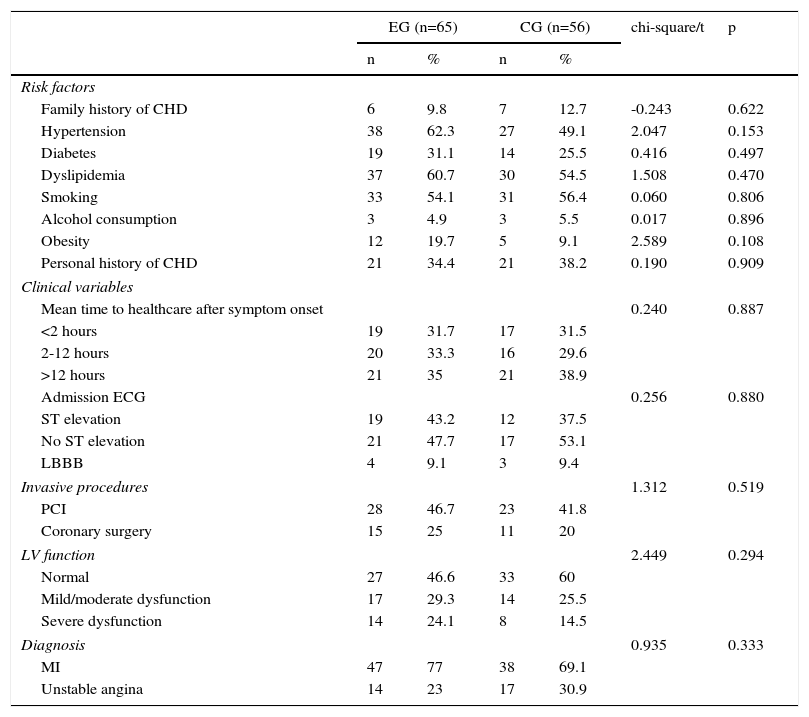
ResultsTables 2 and 3 present the sociodemographic and clinical characteristics of the sample. The groups were equivalent in most sociodemographic variables and all clinical variables, with only a marginally significant difference found for age, the CG being slightly older (66.1±12.6 vs. 61.8±12.1 years).
Sociodemographic characteristics of the study sample and comparison by group.
| Sociodemographic variables | EG (n=65) | CG (n=56) | chi-square/t | p | ||
|---|---|---|---|---|---|---|
| n | % | n | % | |||
| Gender | 0.102 | 0.749 | ||||
| Female | 20 | 31.3 | 16 | 28.6 | ||
| Male | 44 | 68.8 | 40 | 71.4 | ||
| Marital status | 1.020 | 0.600 | ||||
| Married | 50 | 78.1 | 45 | 80.4 | ||
| Widow(er) | 9 | 14.1 | 9 | 16.1 | ||
| Other | 5 | 7.8 | 2 | 3.6 | ||
| Education | 3.785 | 0.286 | ||||
| <4 years | 13 | 20 | 12 | 21.4 | ||
| 4 years | 23 | 35.4 | 27 | 48.2 | ||
| 4-12 years | 18 | 27.7 | 13 | 23.2 | ||
| >12 years | 11 | 16.9 | 4 | 7.1 | ||
| Employment status | 2.266 | 0.322 | ||||
| Employed | 23 | 35.4 | 13 | 23.2 | ||
| Retired | 36 | 55.4 | 38 | 67.9 | ||
| Other | 6 | 9.2 | 5 | 8.9 | ||
| Family status | 1.855 | 0.603 | ||||
| Single | 7 | 10.8 | 4 | 7.1 | ||
| Married | 21 | 32.3 | 23 | 41.1 | ||
| Married with children | 31 | 47.7 | 22 | 39.3 | ||
| Other | ||||||
| M | SD | M | SD | chi-square/t | p | |
|---|---|---|---|---|---|---|
| Age | 61.77 | 12.11 | 66.11 | 12.61 | -1.927 | 0.056 |
CG: control group; EG: experimental group; M: mean; SD: standard deviation.
Clinical characteristics of the study sample and comparison by group.
| EG (n=65) | CG (n=56) | chi-square/t | p | |||
|---|---|---|---|---|---|---|
| n | % | n | % | |||
| Risk factors | ||||||
| Family history of CHD | 6 | 9.8 | 7 | 12.7 | -0.243 | 0.622 |
| Hypertension | 38 | 62.3 | 27 | 49.1 | 2.047 | 0.153 |
| Diabetes | 19 | 31.1 | 14 | 25.5 | 0.416 | 0.497 |
| Dyslipidemia | 37 | 60.7 | 30 | 54.5 | 1.508 | 0.470 |
| Smoking | 33 | 54.1 | 31 | 56.4 | 0.060 | 0.806 |
| Alcohol consumption | 3 | 4.9 | 3 | 5.5 | 0.017 | 0.896 |
| Obesity | 12 | 19.7 | 5 | 9.1 | 2.589 | 0.108 |
| Personal history of CHD | 21 | 34.4 | 21 | 38.2 | 0.190 | 0.909 |
| Clinical variables | ||||||
| Mean time to healthcare after symptom onset | 0.240 | 0.887 | ||||
| <2 hours | 19 | 31.7 | 17 | 31.5 | ||
| 2-12 hours | 20 | 33.3 | 16 | 29.6 | ||
| >12 hours | 21 | 35 | 21 | 38.9 | ||
| Admission ECG | 0.256 | 0.880 | ||||
| ST elevation | 19 | 43.2 | 12 | 37.5 | ||
| No ST elevation | 21 | 47.7 | 17 | 53.1 | ||
| LBBB | 4 | 9.1 | 3 | 9.4 | ||
| Invasive procedures | 1.312 | 0.519 | ||||
| PCI | 28 | 46.7 | 23 | 41.8 | ||
| Coronary surgery | 15 | 25 | 11 | 20 | ||
| LV function | 2.449 | 0.294 | ||||
| Normal | 27 | 46.6 | 33 | 60 | ||
| Mild/moderate dysfunction | 17 | 29.3 | 14 | 25.5 | ||
| Severe dysfunction | 14 | 24.1 | 8 | 14.5 | ||
| Diagnosis | 0.935 | 0.333 | ||||
| MI | 47 | 77 | 38 | 69.1 | ||
| Unstable angina | 14 | 23 | 17 | 30.9 | ||
CG: control group; CHD: coronary heart disease; ECG: electrocardiogram; EG: experimental group; LBBB: left bundle branch block; LV: left ventricular; MI: myocardial infarction; PCI: percutaneous coronary intervention.
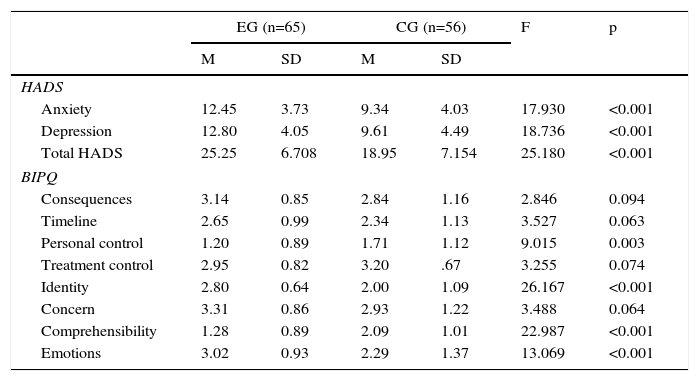
The EG and CG differed at pre-test in most of the psychosocial outcomes (Table 4), although these pre-test differences were controlled for in testing the hypotheses. The CG had lower levels of anxiety (9.34±4.03 vs. 12.45±3.73) and depression (9.61±4.49 vs. 12.80±4.05). Regarding illness cognitions at pre-test, the EG had more negative perceptions of their illness for the personal control, identity, comprehensibility and emotions sub-scales of the BIPQ.
Results of covariance analyses for Hospital Anxiety and Depression Scale and Brief Illness Perception Questionnaire scores at pre-test, with group as factor, controlling for age (n=121).
| EG (n=65) | CG (n=56) | F | p | |||
|---|---|---|---|---|---|---|
| M | SD | M | SD | |||
| HADS | ||||||
| Anxiety | 12.45 | 3.73 | 9.34 | 4.03 | 17.930 | <0.001 |
| Depression | 12.80 | 4.05 | 9.61 | 4.49 | 18.736 | <0.001 |
| Total HADS | 25.25 | 6.708 | 18.95 | 7.154 | 25.180 | <0.001 |
| BIPQ | ||||||
| Consequences | 3.14 | 0.85 | 2.84 | 1.16 | 2.846 | 0.094 |
| Timeline | 2.65 | 0.99 | 2.34 | 1.13 | 3.527 | 0.063 |
| Personal control | 1.20 | 0.89 | 1.71 | 1.12 | 9.015 | 0.003 |
| Treatment control | 2.95 | 0.82 | 3.20 | .67 | 3.255 | 0.074 |
| Identity | 2.80 | 0.64 | 2.00 | 1.09 | 26.167 | <0.001 |
| Concern | 3.31 | 0.86 | 2.93 | 1.22 | 3.488 | 0.064 |
| Comprehensibility | 1.28 | 0.89 | 2.09 | 1.01 | 22.987 | <0.001 |
| Emotions | 3.02 | 0.93 | 2.29 | 1.37 | 13.069 | <0.001 |
BIPQ: Brief Illness Perception Questionnaire; CG: control group; EG: experimental group; HADS: Hospital Anxiety and Depression Scale; M: mean; SD: standard deviation.
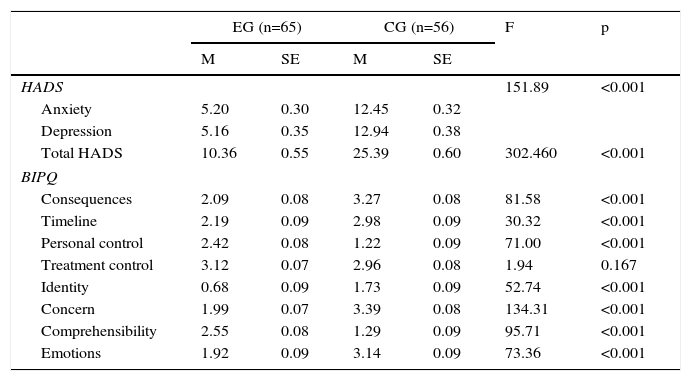
Table 5 shows that the CG presented significantly higher (p<0.001) levels of anxiety and depression at post-test than the EG. The same can be observed for the total HADS score, which was significantly higher than in the EG (p<0.001).
Results of covariance analyses and multivariate covariance analyses for Hospital Anxiety and Depression Scale and Brief Illness Perception Questionnaire scores at post-test, with group as factor, controlling for age and pre-test subscale values (n=121).
| EG (n=65) | CG (n=56) | F | p | |||
|---|---|---|---|---|---|---|
| M | SE | M | SE | |||
| HADS | 151.89 | <0.001 | ||||
| Anxiety | 5.20 | 0.30 | 12.45 | 0.32 | ||
| Depression | 5.16 | 0.35 | 12.94 | 0.38 | ||
| Total HADS | 10.36 | 0.55 | 25.39 | 0.60 | 302.460 | <0.001 |
| BIPQ | ||||||
| Consequences | 2.09 | 0.08 | 3.27 | 0.08 | 81.58 | <0.001 |
| Timeline | 2.19 | 0.09 | 2.98 | 0.09 | 30.32 | <0.001 |
| Personal control | 2.42 | 0.08 | 1.22 | 0.09 | 71.00 | <0.001 |
| Treatment control | 3.12 | 0.07 | 2.96 | 0.08 | 1.94 | 0.167 |
| Identity | 0.68 | 0.09 | 1.73 | 0.09 | 52.74 | <0.001 |
| Concern | 1.99 | 0.07 | 3.39 | 0.08 | 134.31 | <0.001 |
| Comprehensibility | 2.55 | 0.08 | 1.29 | 0.09 | 95.71 | <0.001 |
| Emotions | 1.92 | 0.09 | 3.14 | 0.09 | 73.36 | <0.001 |
BIPQ: Brief Illness Perception Questionnaire; CG: control group; EG: experimental group; HADS: Hospital Anxiety and Depression Scale; M: mean; SE: standard error.
The EG presented significant improvements (all p<0.001) at post-test in illness representations in terms of their perception of illness consequences, timeline, experience of symptoms (identity), concern, emotions, personal control and comprehensibility, whereas the CG presented a less adaptive cognitive profile (Table 5).
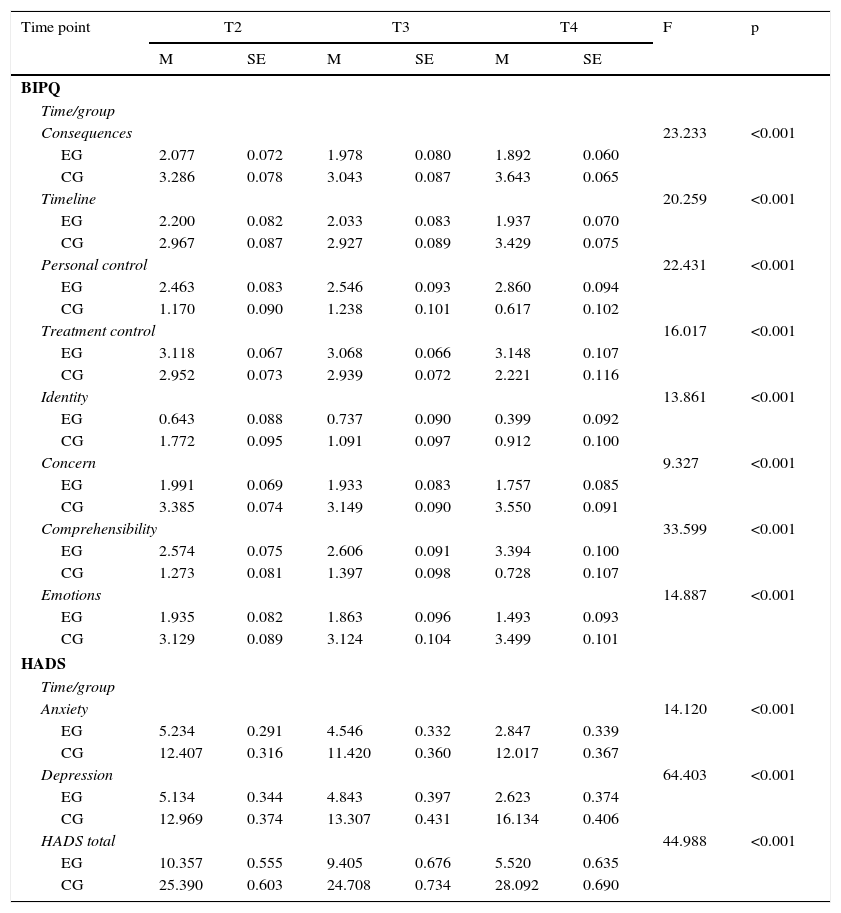
Hypothesis 2: time changes by groupEmotional stateTable 6 presents the results for time/group interaction effects (covariance analyses and repeated measures multivariate covariance analyses) for post-test through the 2-month follow-up changes by group. The EG presented a linear tendency to decrease in terms of anxiety and depression over time, whereas the CG maintained higher anxiety and increased depression with time, especially at two months after hospital discharge. A similar pattern can be observed for the total HADS scores, with a decrease over time in emotional distress for the EG and no change or increase with time in the CG, especially at 2-month follow-up.
Results of repeated measures multivariate covariance analyses for the Hospital Anxiety and Depression Scale and Brief Illness Perception Questionnaire subscale scores, using time and group as factors and controlling for the effects of age and pre-test subscale scores (n=121).
| Time point | T2 | T3 | T4 | F | p | |||
|---|---|---|---|---|---|---|---|---|
| M | SE | M | SE | M | SE | |||
| BIPQ | ||||||||
| Time/group | ||||||||
| Consequences | 23.233 | <0.001 | ||||||
| EG | 2.077 | 0.072 | 1.978 | 0.080 | 1.892 | 0.060 | ||
| CG | 3.286 | 0.078 | 3.043 | 0.087 | 3.643 | 0.065 | ||
| Timeline | 20.259 | <0.001 | ||||||
| EG | 2.200 | 0.082 | 2.033 | 0.083 | 1.937 | 0.070 | ||
| CG | 2.967 | 0.087 | 2.927 | 0.089 | 3.429 | 0.075 | ||
| Personal control | 22.431 | <0.001 | ||||||
| EG | 2.463 | 0.083 | 2.546 | 0.093 | 2.860 | 0.094 | ||
| CG | 1.170 | 0.090 | 1.238 | 0.101 | 0.617 | 0.102 | ||
| Treatment control | 16.017 | <0.001 | ||||||
| EG | 3.118 | 0.067 | 3.068 | 0.066 | 3.148 | 0.107 | ||
| CG | 2.952 | 0.073 | 2.939 | 0.072 | 2.221 | 0.116 | ||
| Identity | 13.861 | <0.001 | ||||||
| EG | 0.643 | 0.088 | 0.737 | 0.090 | 0.399 | 0.092 | ||
| CG | 1.772 | 0.095 | 1.091 | 0.097 | 0.912 | 0.100 | ||
| Concern | 9.327 | <0.001 | ||||||
| EG | 1.991 | 0.069 | 1.933 | 0.083 | 1.757 | 0.085 | ||
| CG | 3.385 | 0.074 | 3.149 | 0.090 | 3.550 | 0.091 | ||
| Comprehensibility | 33.599 | <0.001 | ||||||
| EG | 2.574 | 0.075 | 2.606 | 0.091 | 3.394 | 0.100 | ||
| CG | 1.273 | 0.081 | 1.397 | 0.098 | 0.728 | 0.107 | ||
| Emotions | 14.887 | <0.001 | ||||||
| EG | 1.935 | 0.082 | 1.863 | 0.096 | 1.493 | 0.093 | ||
| CG | 3.129 | 0.089 | 3.124 | 0.104 | 3.499 | 0.101 | ||
| HADS | ||||||||
| Time/group | ||||||||
| Anxiety | 14.120 | <0.001 | ||||||
| EG | 5.234 | 0.291 | 4.546 | 0.332 | 2.847 | 0.339 | ||
| CG | 12.407 | 0.316 | 11.420 | 0.360 | 12.017 | 0.367 | ||
| Depression | 64.403 | <0.001 | ||||||
| EG | 5.134 | 0.344 | 4.843 | 0.397 | 2.623 | 0.374 | ||
| CG | 12.969 | 0.374 | 13.307 | 0.431 | 16.134 | 0.406 | ||
| HADS total | 44.988 | <0.001 | ||||||
| EG | 10.357 | 0.555 | 9.405 | 0.676 | 5.520 | 0.635 | ||
| CG | 25.390 | 0.603 | 24.708 | 0.734 | 28.092 | 0.690 | ||
BIPQ: Brief Illness Perception Questionnaire; CG: control group; EG: experimental group; HADS: Hospital Anxiety and Depression Scale; M: mean; SE: standard error; T2: post-test; T3: 1-month follow-up; T4: 2-month follow-up.
In relation to illness representations, significant time/group interaction effects were observed for all dimensions (all p<0.001, Table 6). Overall, there were more positive illness cognitions in the EG than in the CG, and this advantage was maintained over time. More specifically, patients in the EG perceived less negative consequences of their illness than in the CG, and this perception tended to decrease over time, whereas the CG showed increased perception of negative consequences of their illness after discharge. A similar pattern can be seen in terms of timeline, concern and emotions, indicating an advantage for the EG over time. Identity perception tended to decrease with time in both groups, although the CG reported more symptoms associated with their illness than the EG. The perception of personal control, treatment control and comprehensibility increased over time in the EG, whereas these dimensions tended to decrease in the CG, especially at 2-month follow-up.
DiscussionThis study aimed to test the efficacy of a brief in-hospital psychosocial intervention directed at improving emotional and cognitive outcomes for patients with ACS. The results demonstrate significant benefits for the EG in terms of less anxiety and depression and more positive illness representations after the intervention, in comparison to the CG, who received standard medical care. These results are even more significant given the fact that the EG had a less favorable psychosocial profile at pre-test than the CG. These results were independent of patients’ age and baseline scores on the psychosocial variables studied. The advantages of the intervention for the EG were particularly noticeable at two months post-discharge, suggesting that the effects of the intervention lasted into the rehabilitation period, counteracting the psychosocial deterioration that was observed in the CG.
The positive impact of this intervention in terms of depressive symptoms is important bearing in mind the predictive effect of depression on cardiovascular mortality after ACS.21,22 The intervention program sought to prevent the increase in both anxiety and depression associated with post-ACS rehabilitation, not only by promoting education about ACS and its treatment but also by increasing psychosocial skills (adaptive cognitive and cognitive-behavioral coping strategies) used to reduce the negative psychological impact of the acute event. Implementation of behavioral and cognitive coping strategies to deal with emotional difficulties associated with a cardiac event is an active component of many multimodal psychological intervention programs, and is believed to be a factor directly related to reducing the recurrence of ACS.23,24
Our results also support the effectiveness of the intervention program in changing disease cognitions. Patients in the EG had more positive illness representations after the intervention, and had perception of greater personal control and a greater understanding of the meaning of their disease. Indeed, one of the main aspects of the intervention program was education regarding disease cognitions, providing information that could correct beliefs and help patients become more active participants in the process of illness and treatment. The positive results in terms of increased understanding of the disease are in agreement with those obtained in other studies, which report a positive effect of a brief hospital intervention at this level.16 From the standpoint of decreased cardiac vulnerability, the significant increase in understanding of the disease is also important, since there are indications of an association between good understanding of the disease and increase in therapeutic adherence.9 Increased perception of personal control also has important clinical implications, as several studies have shown that a strong sense of control in coronary patients is an important predictor of improved emotional state25 and quality of life in the context of CR after ACS.26
Research into the factors predicting a lack of adherence to CR has pointed to the importance of psychosocial aspects, such as patients’ illness cognitions and emotional state.27 De Vos et al.6 investigated patient compliance with CR and reasons for refusing or abandoning programs, finding that the main reasons for not completing CR programs were other physical problems, patients’ belief that they could handle their own problems, and the cost of rehabilitation. The literature suggests that patients’ emotional state (e.g. anxiety and depression) and illness representations need to be assessed early on as a way of optimizing adherence to and benefits of CRP, promoting better psychosocial adaptation in the post-ACS period.5,28–30. Patients’ beliefs about their illness and treatment have been found to predict clinical and psychological outcomes post-discharge.14 There is evidence that the perception that one can have some control over the course of illness, as well as belief in treatment success, are determining factors in recovery.31
This study presents evidence that a brief psychosocial intervention undertaken during hospitalization presents considerable benefits in improving psychological morbidity and adaptation to post-ACS rehabilitation. The intervention administered is of low financial cost, carries low patient and professional burden (less than three hours in total duration), and can be easily implemented in routine healthcare. This type of intervention can be particularly useful in countries such as Portugal that have fewer medical and economic resources.
The most favorable time for psychological intervention, in terms of effectiveness, is at hospitalization, when patients are most accessible to this type of intervention and to lifestyle changes. This has been confirmed by international studies and trials evaluating the efficacy of psychological intervention in post-ACS rehabilitation16,31 and also by our previous study that evaluated the effectiveness of a psychological intervention program in phase II of cardiac rehabilitation.20,32 The fact that patients are close in time to the acute coronary event, are in a supportive environment, and are physically present and have time available for participation in the intervention, creates a window of opportunity that our intervention appears to have optimized. A psychological approach during hospitalization is essential to identify and assess the representations of disease and the patient's emotional state, which significantly influence the quality of the post-ACS rehabilitation process.
The current study has some limitations. We did not assess whether the positive gains in psychosocial adjustment in the EG translated into better cardiac function and physical health than in the CG. However, it is generally accepted that psychosocial maladjustment (particularly anxiety and depression or depressive symptoms) are independent factors of worse prognosis in post-ACS patients,33–37 involving neuroendocrine and inflammatory mechanisms as well as behavioral factors.38 Furthermore, a longer follow-up would establish whether these positive effects in adjustment persist over a longer period of time. It is important to replicate this intervention study in other hospital-based coronary care units and to include longer follow-up periods and a more diverse array of outcomes, both clinical (e.g. recurrence of ACS) and behavioral (e.g. lifestyle changes).
Despite these limitation, our results highlight the positive impact of a brief psychological intervention in phase I of a CR program, targeting recognized psychological risk factors for ACS rehabilitation and ultimately for cardiac prognosis.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interestThe authors have no conflicts of interest to declare.
