



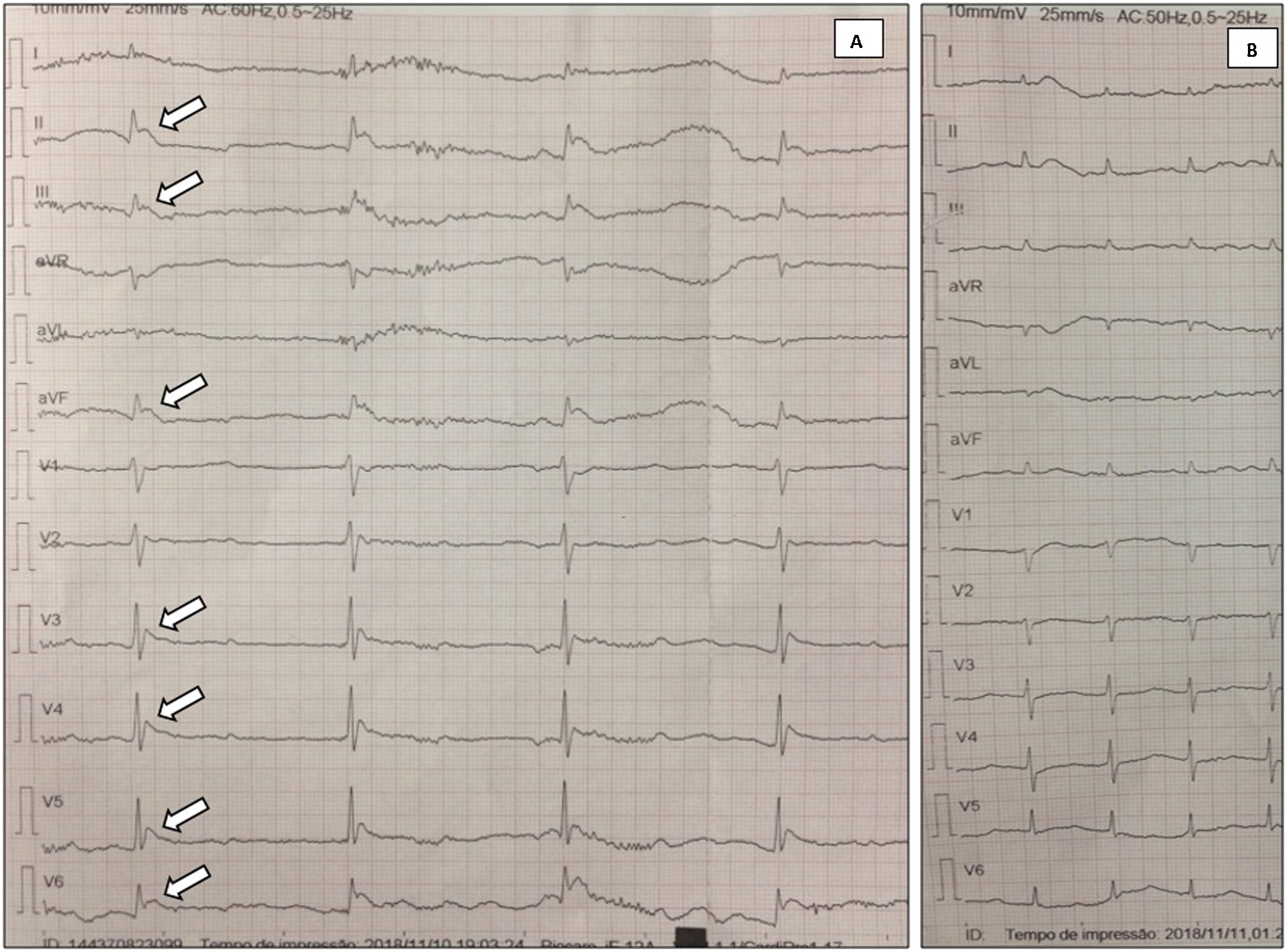
A 59-year-old man with a history of alcohol abuse was found fallen and unconscious at his home in the winter. He was severely hypothermic (26°C) and with poor peripheral perfusion. The electrocardiogram showed heart rate of 34 bpm, complete atrioventricular block and inferolateral J-wave elevation, suggestive of Osborn waves (Figure 1A).
Blood tests showed rhabdomyolysis; toxicology and alcohol screens were negative and brain computed tomography and echocardiogram were normal.
After re-establishment of normothermia with heated intravenous fluids and external warmer, restoration of sinus rhythm and resolution of the Osborn waves was observed (Figure 1B).
An elevated J point in hypothermia (Osborn wave) was first described by John Osborn in 1953. Although it has been considered pathognomonic of hypothermia, it may also be present in other conditions, such as electrolyte disturbances or brain injuries. Other typical electrocardiographic abnormalities in hypothermia include prolonged PR/QT/QRS duration, conduction abnormalities and atrial or ventricular arrhythmias.
Considering the similarity of Osborn waves to other forms of J-point elevation, such as myocardial infarction or Brugada syndrome, this may lead to an incorrect diagnosis, especially in the setting of an acute event, which reinforces the importance of knowing this pattern and its cause.
Conflicts of interestThe authors have no conflicts of interest to declare.
