

L waves are an unusual finding in the analysis of mitral valve pulsed-wave Doppler. This wave is recorded as flow between the left atrium and left ventricle during diastole, due to elevated left ventricular (LV) filling pressures.1–3 In this situation, triphasic mitral filling can be observed, with the presence of mid-diastolic L waves.
We present the case of a 71-year-old female with preserved LV ejection fraction (LVEF) and moderate ventricular hypertrophy secondary to hypertensive cardiomyopathy, according to a cardiac magnetic resonance study performed the year before. The patient had an episode of acute pulmonary edema during an admission for malaria, with complications of fever, acute kidney disease and hypertensive crisis. During the initial assessment, a transthoracic echocardiogram was performed, which showed high LV filling pressure (E/E′ ratio 23), systolic pulmonary pressure of 60 mmHg estimated by tricuspid regurgitation Doppler, and L waves on mitral pulsed-wave Doppler (Figure 1). Laboratory tests showed NT-proBNP of 1962 pg/ml.
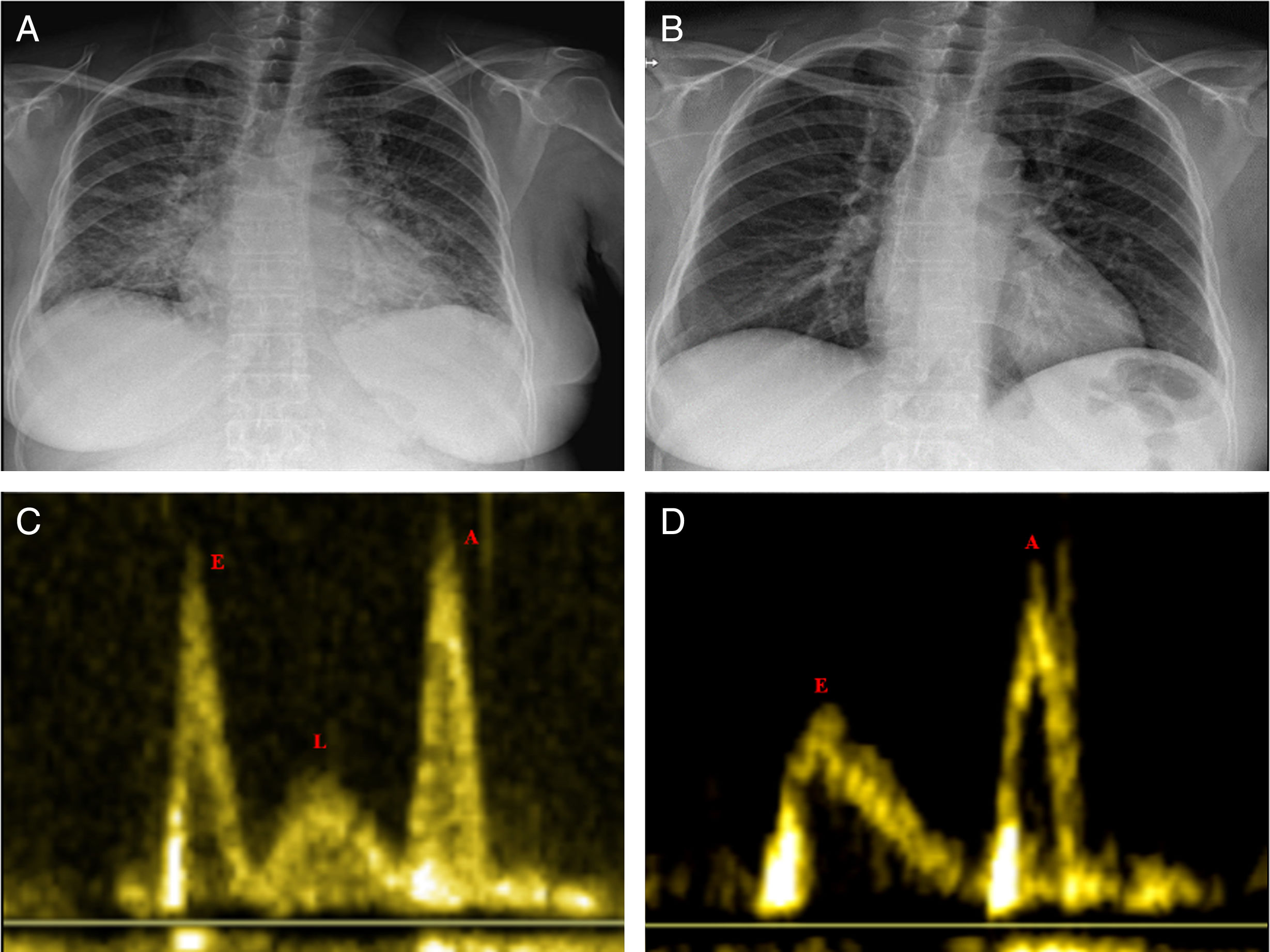
After treatment with antihypertensive drugs and diuretics, following diuresis of 12 l in three days, the patient had normal LV filling pressure (E/E′ ratio 12) and systolic pulmonary pressure of 32 mmHg, and the L wave had disappeared on the echocardiogram, which showed an impaired relaxation pattern in LV filling (EVideos 1 and 2), and a decrease in left atrial volume (from 52.1 to 31.7 ml).
The patient was discharged in good condition after recovery of renal function and adjustment of antihypertensive therapy.
In this paper, we report the presence of L waves during an episode of acute pulmonary edema in a patient with preserved LVEF, in the context of high LV filling pressure. Recognizing this pattern of diastolic filling can be helpful in the rapid diagnosis and treatment of similar cases of heart failure.
Conflicts of interestThe authors have no conflicts of interest to declare.
