






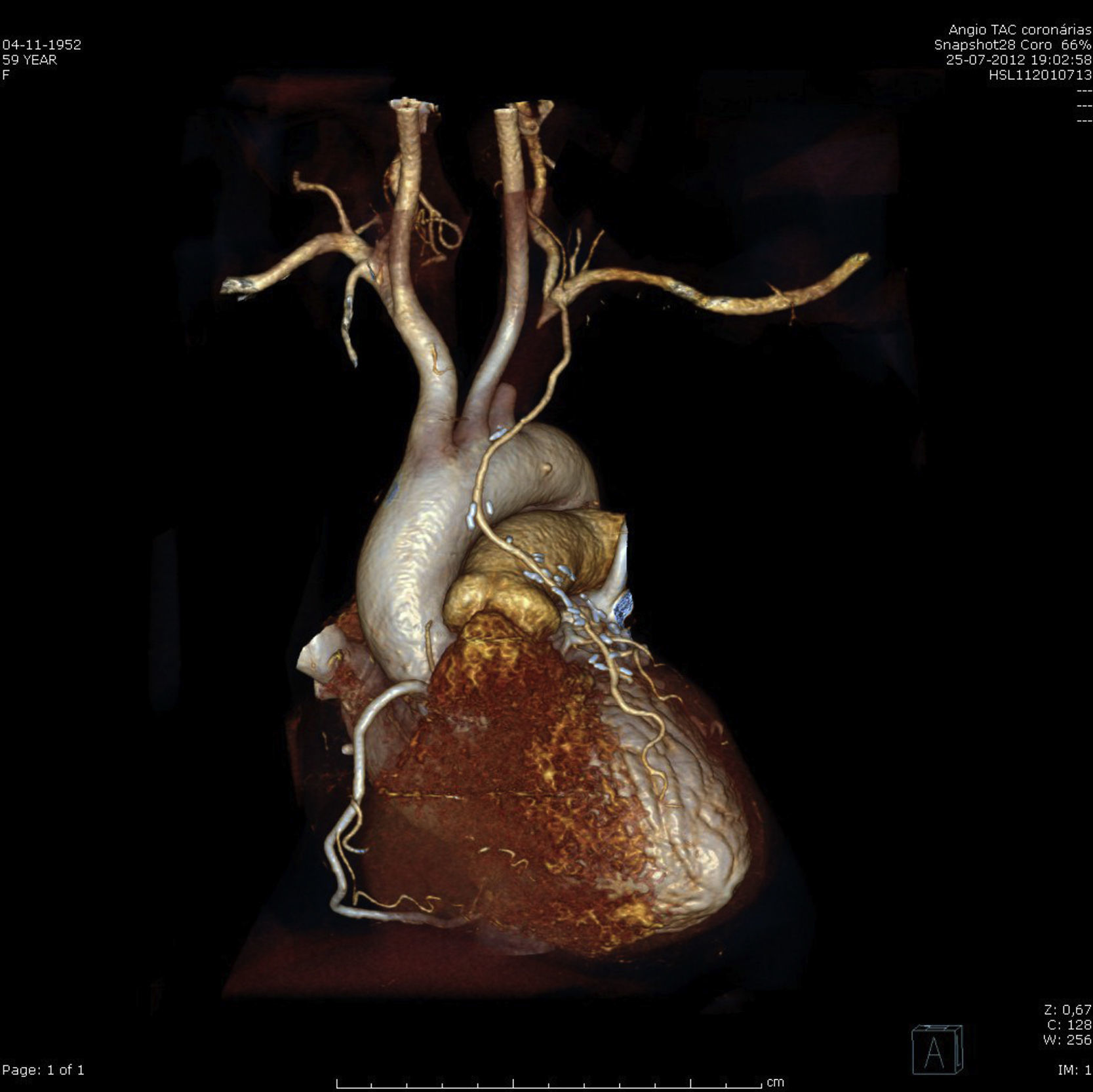
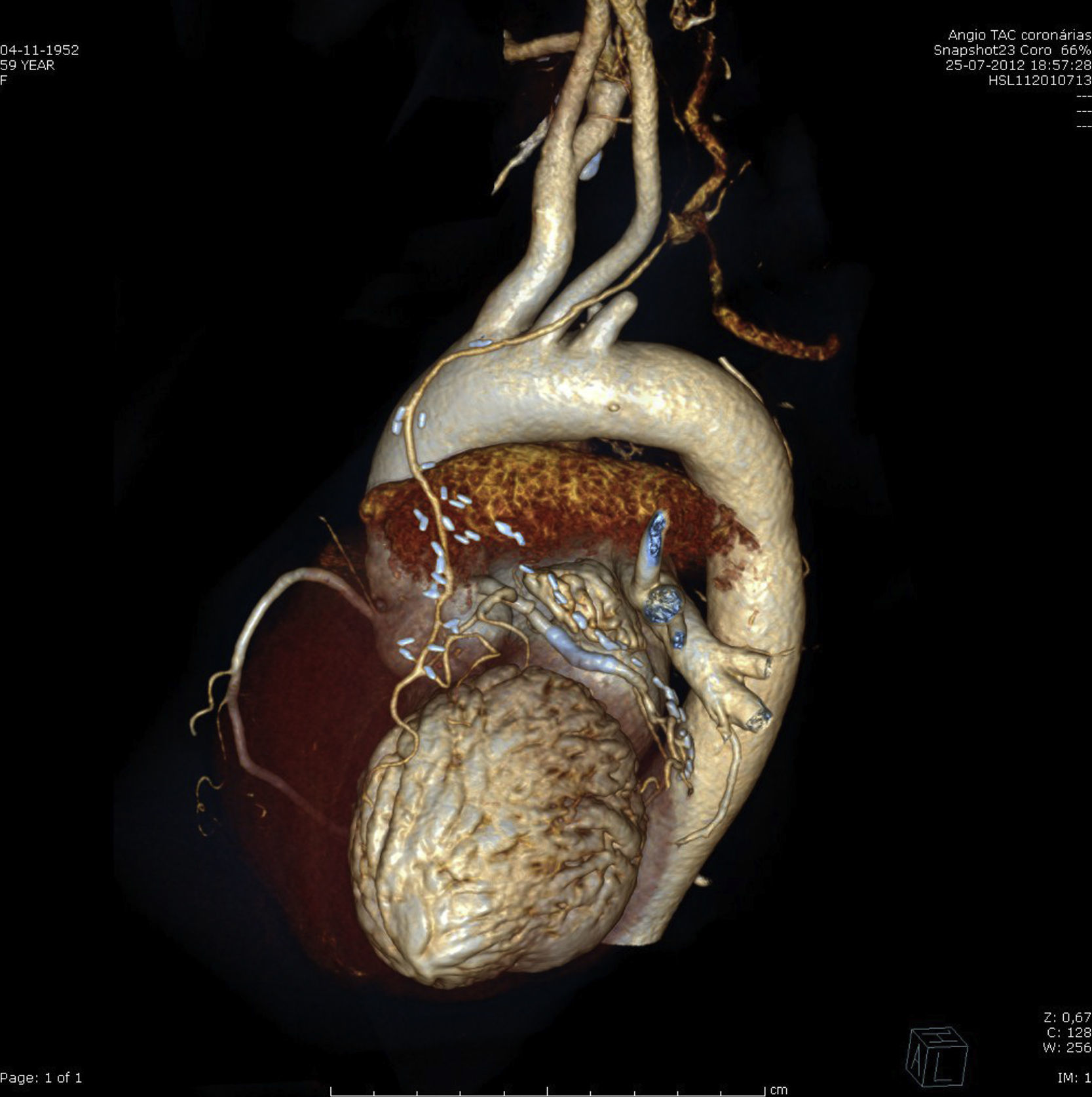
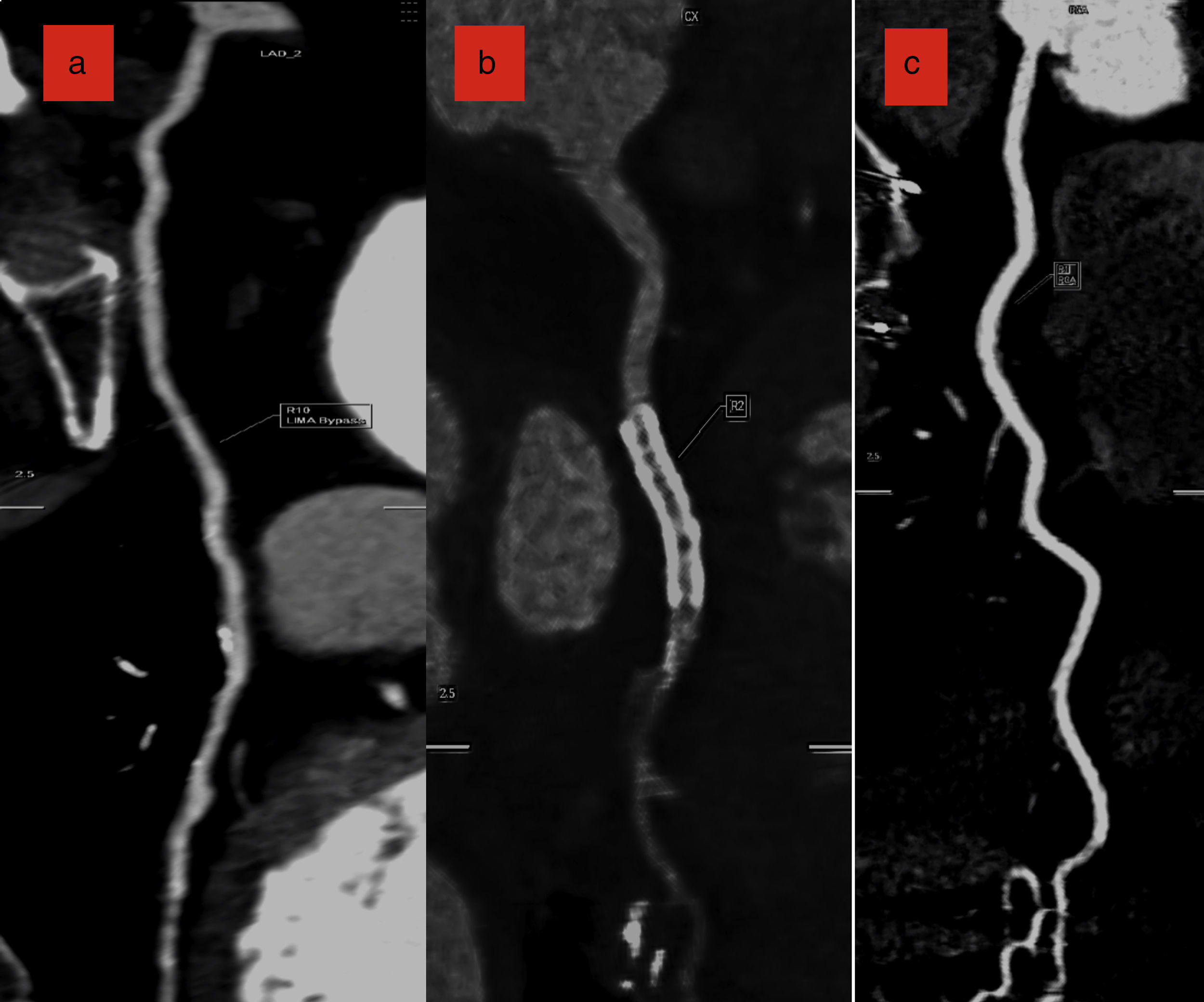
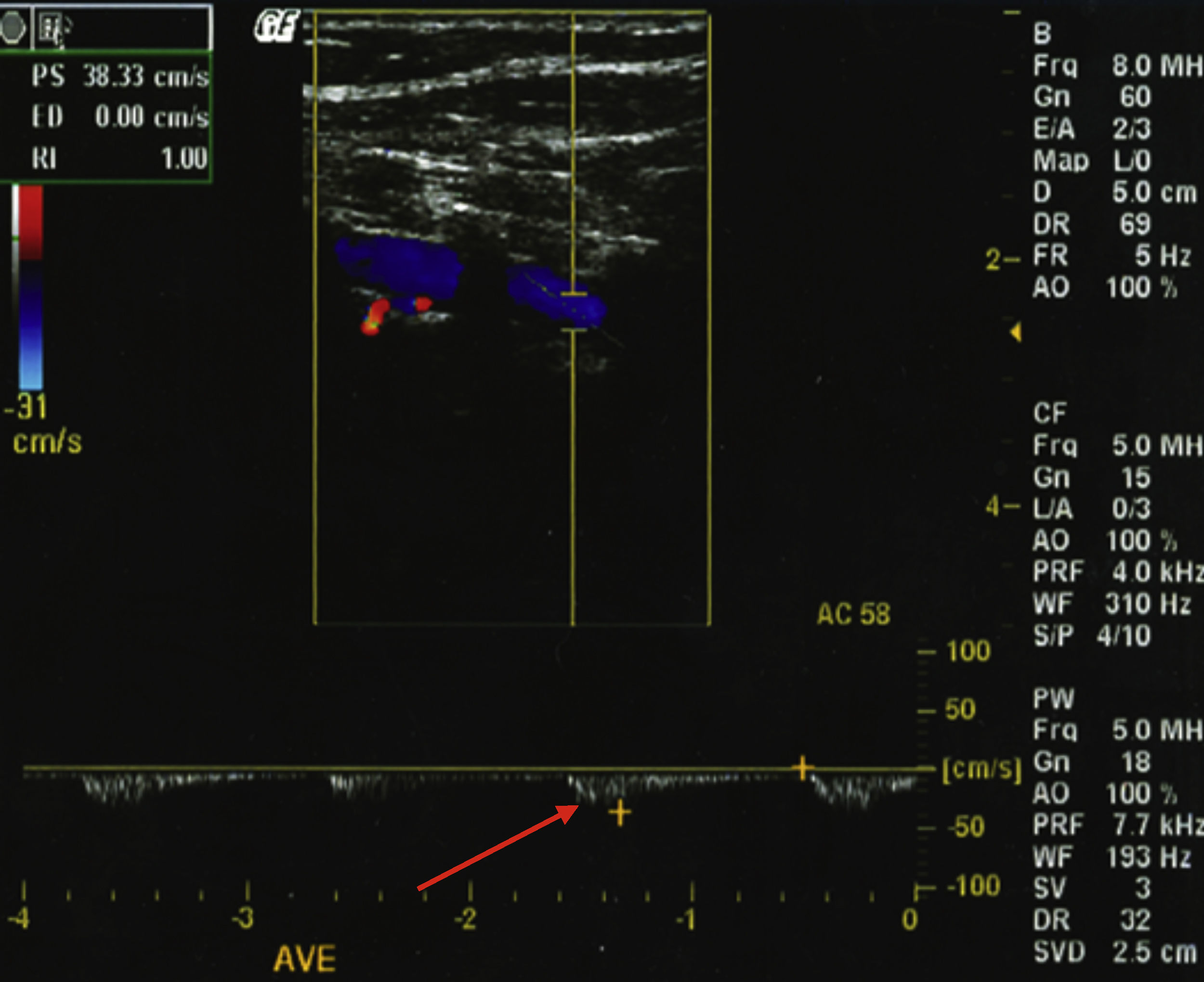
A 59-year-old woman with type 2 diabetes and two-vessel disease had undergone double coronary bypass grafting (CABG) five years previously, with left internal mammary artery (LIMA) to left anterior descending (LAD) artery and free radial graft (Y type), from LIMA to obtuse marginal (OM). Three months ago, the patient began to suffer angina and episodes of dizziness after upper limb exercise, followed by a lateral wall myocardial infarction one month ago. Urgent femoral catheterization revealed thrombotic occlusion of the circumflex (Cx) artery; the LAD had an old occlusion and the LIMA could not be catheterized. The right coronary artery (RCA) was normal. Primary angioplasty of the culprit Cx was performed and two bare-metal stents were deployed. The acute chest pain resolved, but angina and dyspnea recurred one week later. Physical examination revealed absent pulses in the left arm. Cardiac CT angiography revealed abrupt occlusion of the left subclavian artery 1.8cm after its origin, proximal to the LIMA and the ipsilateral vertebral artery. Both these arteries supplied a scant flow to the axillary artery (Figures 1 and 2), but the LIMA was well contrasted, with a good anastomosis to the mid LAD (Figures 1, 2 and 3a). The radial (LIMA to OM) anastomosis was totally occluded, only the path of the metal clips being visible (Figure 2). The Cx stent was patent with no signs of restenosis, and the RCA was normal (Figure 3b and c). The right brachiocephalic and left carotid arteries were normal (Figures 1 and 2). A triplex Doppler scan revealed reversal of left vertebral artery flow (Figure 4). A diagnosis of coronary-vertebral subclavian steal syndrome was made.
Coronary and/or vertebral subclavian steal syndrome is a late complication of CABG, occurring in patients with pre-existing subclavian atherosclerotic disease. It is unclear whether the surgical procedure itself accelerates the development of lesions in the subclavian artery, due to enhanced local flow and consequent endothelial shear stress.1,2 Systematic bilateral blood pressure measurement is mandatory prior to CABG, to exclude subclavian stenosis.
In this case, a large CT acquisition window was used, ranging from the middle neck region to the diaphragm, to ensure good anatomical coverage, particularly of the proximal supra-aortic vessels, in preparation for possible future surgery. Since the left carotid artery was disease-free, a carotid-left axillary shunt was proposed, without further invasive investigations.
Ethical responsibilitiesProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data and that all the patients included in the study received sufficient information and gave their written informed consent to participate in the study.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interestThe authors have no conflicts of interest to declare.
