




The European Society of Cardiology (ESC) Core Curriculum for the Cardiologist, first published in 2006, followed by revisions in 2008 and 2013, provides a training framework outlining the requirements and clinical competencies necessary to become a certified cardiologist in Europe. It aims at a progressive standardization and harmonization of the content and quality of training in cardiology within the European Union (EU) member States and other European countries. Upon completion of the curriculum, the trainee should be able to act independently as a cardiology expert in the treatment of cardiovascular (CV) patients, keeping in mind that there are subspecialities within cardiology that require further subspeciality training after certification.
Since 2013, the practice of cardiology has changed substantially; in order to reflect modern cardiology. The 2020 update was a joint effort between the ESC and the European Union of Medical Specialists leading for the first time to a single integrated document. This revision was chaired by Professor Felix C. Tanner (University Heart Center, Zurich, Switzerland), who was given the opportunity to assemble a widely representative task force. It included contributors from the ESC Education Committee and liaison officers of the ESC associations, members of the ESC board and representatives of the ESC Working Groups and of national cardiology societies. Additionally, representatives from the Young Cardiology Community and patients themselves were for the first time involved in this revision and provided different and valuable perspectives. All members of the task force had the opportunity to an iterative process contribute along an iterative process which employed online Delphi surveys and in-person discussions and meetings and to review the updated document before its publication, which was simultaneous with its presentation at the ESC Congress 2020.1,2
What is new in the 2020 edition – trust in trainingBesides the updated definition of the core areas needed for the practice of Cardiology, one of the main changes in this 2020 curriculum is the implementation of Entrustable Professional Activities (EPAs) to describe clinical competencies. This concept has been increasingly used by medical educators throughout the world and the name arises from the fact that trust is a central aspect of learning. During training, trainees progressively acquire knowledge, skills, and attitudes while, at the same time, trainers develop increasing trust in their trainees. This process is often subconscious, but EPAs make it conscious and formalize it. EPAs are defined as units of professional activity or clinical competence that a trainee can be trusted to perform in a given healthcare context, once an appropriate competence level has been demonstrated.
This 2020 revision is based on ESC clinical practice guidelines and covers the ESC topic list. It comprises 62 EPAs organized in 9 chapters (The Cardiologist in the wider context; Imaging; Coronary artery disease; Valvular heart disease; Rhythm disorders; Heart failure; Acute cardiovascular care; Prevention, rehabilitation, and sports; Cardiac patients in other settings). Each EPA presents clear definitions of knowledge, skills and attitudes needed for its completion, as well as assessment tools and expected levels of competence.
In past versions of the Core Curriculum, a fixed number of investigations and techniques was defined and a trainee had to become competent in each one of them. Nevertheless, there is now much evidence confirming the empirical notion that each trainee requires different amounts of practice to achieve expertise. In other words, the number of times a procedure has been performed is not relevant if the trainee is able to perform it independently. In line with the 2013 ESC Core Curriculum, the 2020 update foregoes this concept of set numbers and focuses on the level of entrustment. While previous versions defined three levels of competence, each of the EPAs and each of the investigations and techniques performed in Cardiology now have five entrustment levels, corresponding to the increasing independence reached by the trainee: observing the activity (level 1), activity performed under direct supervision (level 2), activity performed under indirect supervision (level 3), activity performed with distant supervision (level 4), and being able to perform the activity independently and supervise others (level 5).
Furthermore, the 2020 update integrates the various professional roles of the cardiologist in the clinical context (CanMEDs roles) regarded as necessary to be competent both generally as a cardiologist (first chapter) and specifically in each EPA.
Globally, these changes enable more flexibility in the training and assessment of trainees and focus on skills in a clinical context (Table 1).1,2
CanMed roles and levels of independence for each entrustable professional activities and each investigation, from level 1 to level 5: (1) Observe; (2) Direct supervision; (3) Indirect supervision; (4) Distant supervision; and (5) Able to teach (no supervision). Adapted from reference 2, with permission.
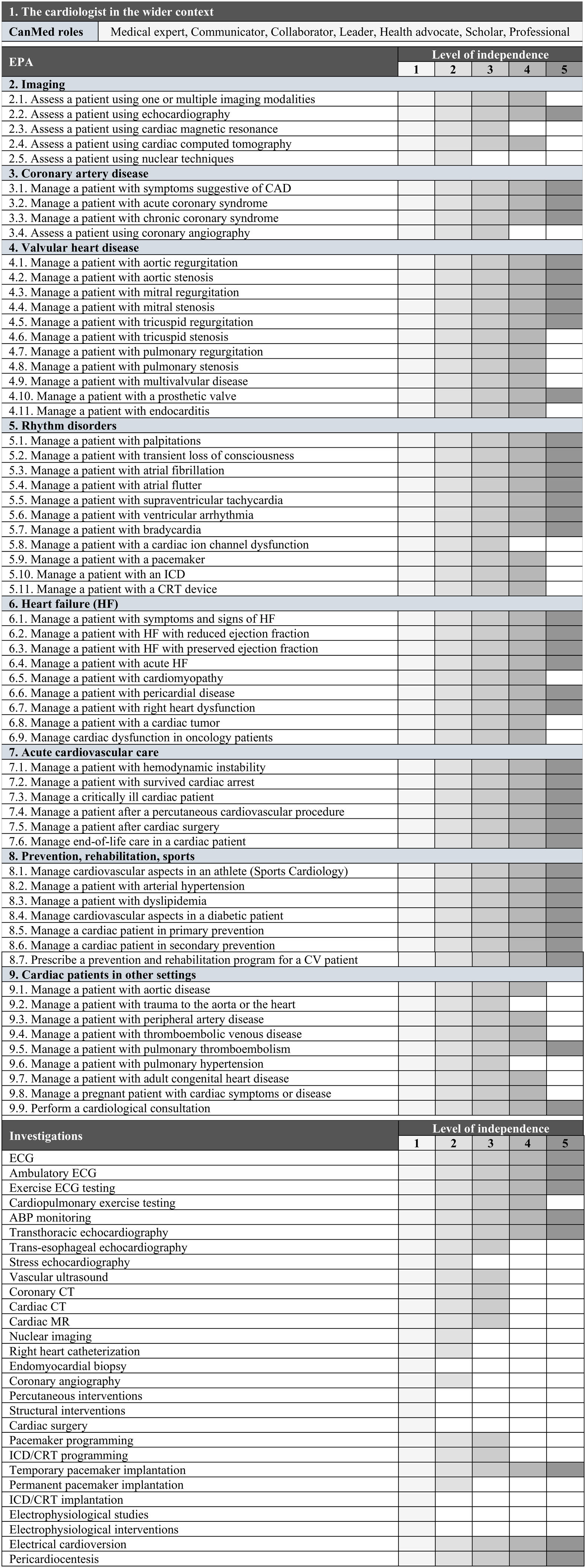
ABP: ambulatory blood pressure; CAD: coronary artery disease; CT: computerized tomography; CV: cardiovascular; ECG: electrocardiogram; HF: heart failure; ICD/CRT: implantable cardioverter defibrillator/cardiac resynchronization therapy devices; MR: magnetic resonance.
The document also updates the requirements for trainees, trainers, training programs and institutions. While the main responsibilities lie with the trainee, trainers should, for example, have their role recognized by national authorities and undertake specific training and continuous professional development in educational supervision and assessment. Training institutions should provide a supportive learning environment, not only through adequate clinical experience but also by allowing each trainee time for scheduled, structured learning.1
Cardiology training in PortugalThe Portuguese Cardiology training program was first published in 1997 and was updated in 20113. Currently, the program consists of one year of General Training, followed by one year of Internal Medicine and General Intensive Care and four years of Cardiology (Table 2).
Portuguese Cardiology Training Program.
| Rotation | Duration | Minimum numbers |
|---|---|---|
| General Training | 12 months | - |
| Internal Medicine | 8 months | - |
| General Intensive Care | 3 months | - |
| Clinical Cardiology | 11 months | - |
| Echocardiography | 6 months | 350 transthoracic echocardiography exams50 transesophageal echocardiography exams20 stress echocardiography exams |
| ECG and Ambulatory Monitoring | 3 months | 300 stress ECG tests200 Holter tests50 ABPM tests |
| Cardiac Intensive Care | 5 months | - |
| Interventional Cardiology | 5 months | 300 diagnostic coronary angiographies100 interventional procedures |
| Cardiac Pacing and Electrophysiology | 4 months | 25 temporary pacemaker implantations50 permanent pacemaker implantations20 ICD/CRT implantations50 pacemaker/ICD programming50 electrophysiological studies |
| Nuclear Cardiology, Cardiac MR, and Cardiac CT | 3 months | 50 nuclear scans20 cardiac MRI exams20 cardiac CT exams |
| Congenital Heart Disease | 2 months | - |
| Cardiac Surgery | 2 months | - |
| Optional Rotation | 3 months | - |
ABPM: ambulatory blood pressure monitoring; CT: computerized tomography; ECG: electrocardiogram; ICD/CRT: implantable cardioverter defibrillator/cardiac resynchronization therapy devices; MR: magnetic resonance.
This training aligns with the 2008 version of the ESC Core Curriculum, particularly regarding the minimum numbers for each technique/exam. The 2013 version was the first not including a minimum or optimal number of procedures to be undertaken, while setting level of competences (I, II or III) for each technique. As stated in the document “the number of procedures engaged by trainees is important but is not in itself a robust measure of competence”.4 Given that the 2020 update further develops this concept, it is fair to say the Portuguese training program should also be updated.
Nonetheless, the sole published data regarding satisfaction of Cardiology trainees in Portugal reported high levels of expectations achieved with the specialty and that most of the trainees would choose the same specialty again. However, one should take into account that this study is from 2015; only 14% of trainees participated in the survey; and Cardiology was the specialty whose trainees most considered the possibility of emigration.5
At present, based on the opinion of many Portuguese Cardiology trainees and trainers, the duration and the minimum numbers defined in many of the rotations are not adequate in view of current practice in Cardiology. Overall, and taking the 2020 ESC Core Curriculum into consideration, the duration of some rotations must be reviewed to fully accomplish the proposed EPAs. The evaluation process at the end of the training program is also up for debate. For example, while other specialties in Portugal have their own evaluation grid, the absence of a strict and objective grid in Cardiology leads to a lack of standardization and doubts regarding inequities among training centers and final evaluations.
According to their electoral agenda, the newly appointed board members of the College of Cardiology of the Portuguese Medical Association aim to soon update the training program and revise the evaluation method, most certainly using the 2020 ESC Core Curriculum framework.
Conflicts of interestFelix C. Tanner and Lino Gonçalves are authors of the ESC Core Curriculum 2020 and Kevin Domingues contributed to its development as a Young Cardiology Community Representative.
Maria João Vidigal Ferreira and Miguel Mendes are members of the board of the College of Cardiology of the Portuguese Medical Association.
