





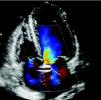

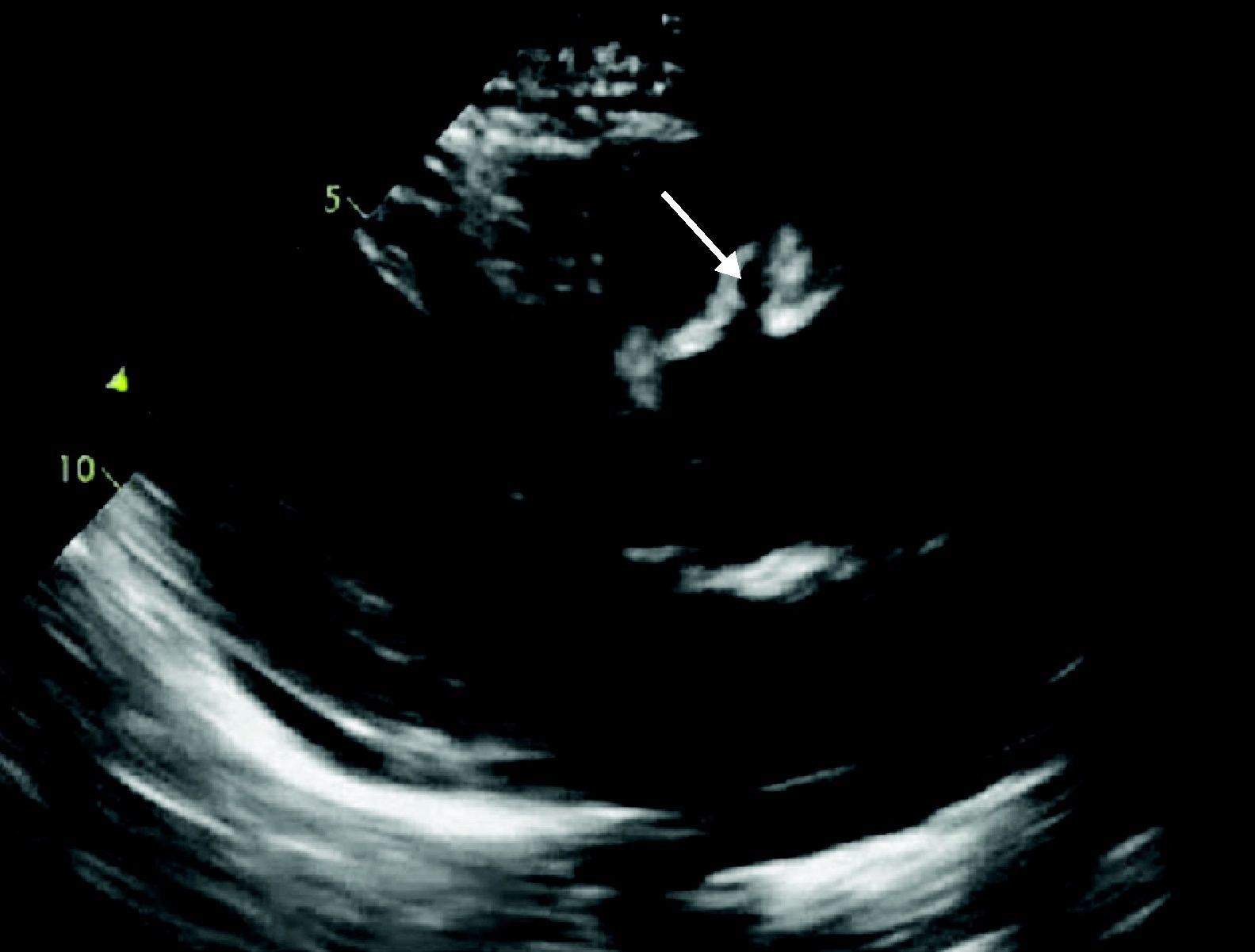
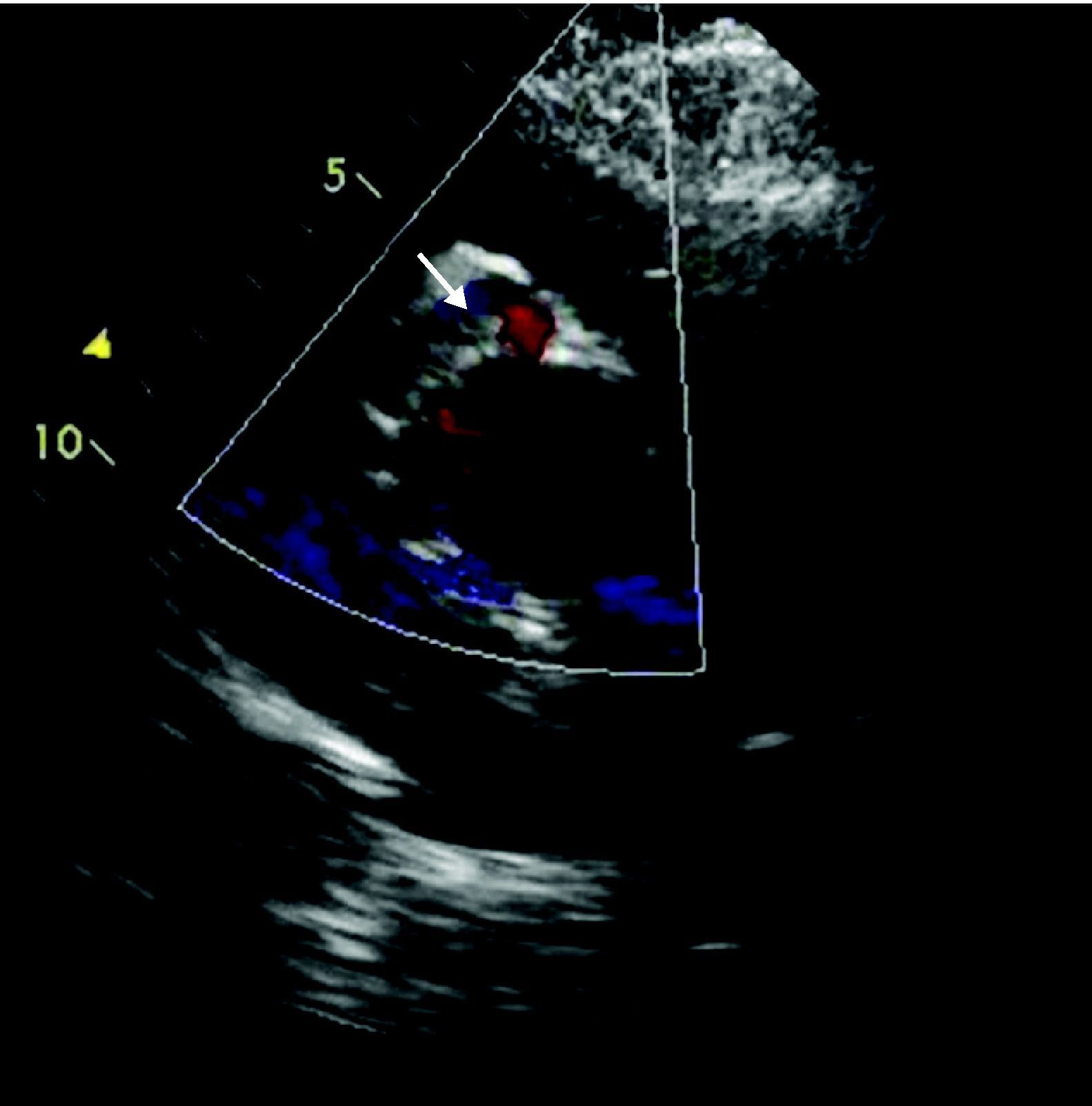
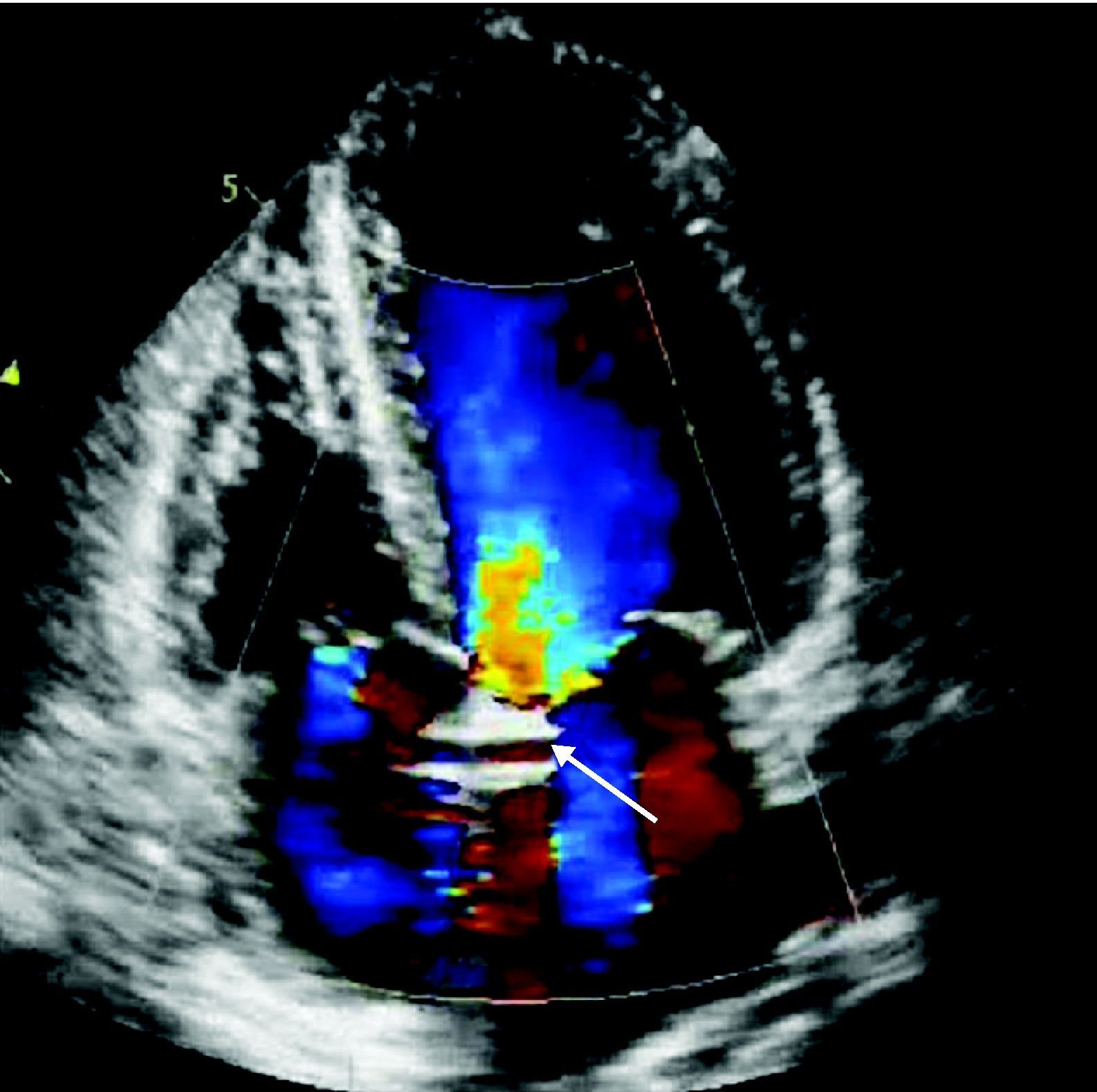
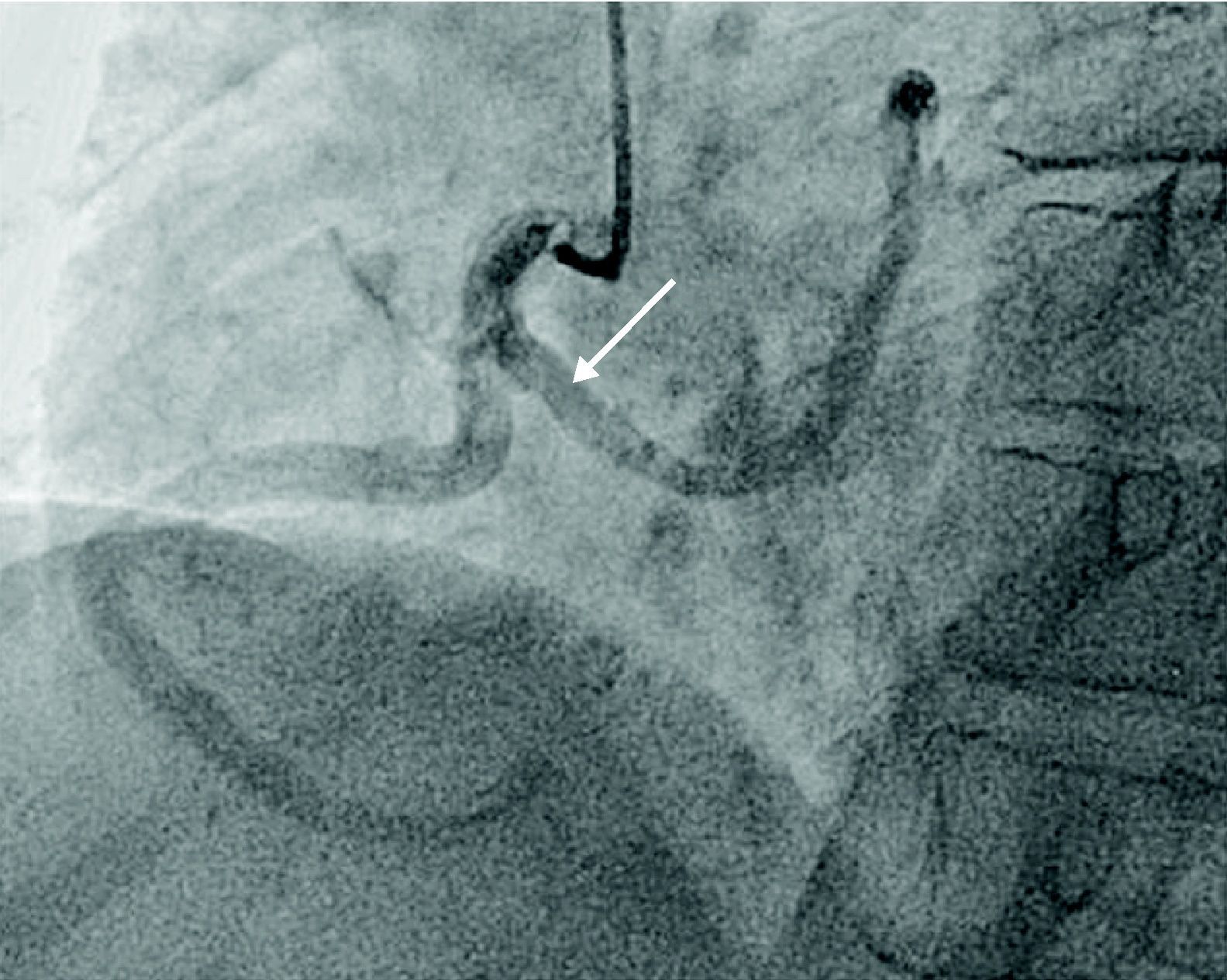
A 67-year-old woman with a history of scleroderma and hypertension but with no previous cardiac symptoms was hospitalized for assessment of systemic sclerosis. Physical examination revealed a grade II/VI systolic murmur on the apex; the electrocardiogram showed sinus rhythm and left anterior bundle branch block. Left parasternal long-axis echocardiography revealed an anomalous tubular image in continuity with the anterior wall of the ascending aorta (Fig. 1), while in parasternal short-axis view the same tubular structure was seen encircling the aorta (Fig. 2). In apical 4-chamber view, a tubular image, 2 mm in diameter and 42 mm in length, was observed crossing the atrial septum; its origin and end were not identified. Color Doppler echocardiography showed flow in its interior (Figs. 3 and 4), which raised the suspicion that it was a vascular structure, and cardiac catheterization was accordingly performed, which revealed anomalous origin of the left coronary artery (LCA) from the proximal segment of the right coronary artery, with an epicardial course anterior to the aorta (Fig. 5). The echocardiographic findings, most often associated with scleroderma, are pulmonary hypertension and pericardial involvement, including fibrinous pericarditis. There are no reports in the literature of an association between scleroderma and anomalous coronary artery origin, and hence this case may be simply a coincidence. Origin of the LCA from the right coronary ostium is found in only 0.15%1 of the population and is associated with sudden death.2

The authors have no conflicts of interest to declare.
Please cite this article as: Faria R, et al. Imagem tubular «transversal ao septo inter-auricular». Rev Port Cardiol 2012. doi:10.1016/j.repc.2012.01.010.
