



We report the interesting case of a rare form of presentation of rupture of the ascending aorta with formation of a pseudoaneurysm, diagnosed following the development of a large mass on the surface of the chest over a period of about eight months. Serological tests were positive for syphilis. Echocardiography and computed tomography angiography were essential to confirm the diagnosis and therapeutic management.
Cardiovascular syphilis is a rare entity since the discovery of penicillin. Rupture of an aortic aneurysm with formation of a pseudoaneurysm is a potentially fatal complication.
The postoperative period was uneventful and the patient was discharged from hospital within days of surgery.
Relata-se o interessante caso de uma rara forma de apresentação de rotura da aorta ascendente com formação de um pseudoaneurisma, diagnosticado por manifestar-se como uma grande massa tumoral na superfície do tórax com evolução clínica de, aproximadamente, oito meses. Provas sorológicas foram positivas para sífilis. Ecocardiografia e angiotomografia foram fundamentais na confirmação diagnóstica e orientação terapêutica.
Sífilis cardiovascular é uma entidade rara após a descoberta da penicilina. Dilatação aneurismática rota da aorta com formação de um pseudoaneurisma é uma complicação potencialmente fatal.
O paciente evoluiu sem intercorrências no período pós-operatório, recebendo alta hospitalar dias após o procedimento cirúrgico.
Aortic pseudoaneurysm is a serious and potentially fatal condition, characterized by accumulation of blood and connective tissue outside the vessel wall. It occurs following rupture of at least one of the layers of the aortic wall, which is contained by the other layers or by adjacent mediastinal structures, leading to the formation of an extraluminal aneurysmal sac that communicates with the true lumen through a narrow neck.
The authors describe the interesting case of a rare form of presentation of rupture of the ascending aorta with formation of a pseudoaneurysm, diagnosed following the development of a large mass on the surface of the chest over a period of about eight months. Echocardiography and computed tomography were essential to confirm the diagnosis and therapeutic management.
Case reportA 54-year-old man, white, sought medical assistance due to a growing mass on his chest over a period of around eight months, associated with non-radiating, throbbing dorsal thoracic pain and headache; the pain was initially mild, progressing to moderate, relieved by ibuprofen. He reported difficulty swallowing but no other symptoms, including chest trauma, acute intense pain or previous infection. He had stopped smoking and drinking alcohol (previously high daily intake) after the onset of symptoms. He was unaware of any comorbidities. On physical examination, the patient was in good general condition, eupneic, with normal color skin and mucosa; there was a large mass on the left anterior chest, around 15 cm in diameter and pulsatile on palpation (Figure 1). Heart rate, blood pressure and pulses were normal. There were no neurological changes. Cardiac auscultation was normal; pulmonary auscultation revealed reduced breath sounds in the left lung base.

Following admission, the patient was medicated with an oral beta-blocker (propranolol). A chest X-ray in posteroanterior view showed mediastinal enlargement and elevation of the base of the left hemithorax, suggestive of diaphragmatic eventration. The electrocardiogram was normal.
Transthoracic (Figure 1) and transesophageal echocardiography revealed aneurysmal dilatation of the distal portion of the ascending aorta and aortic arch, 93 mm at its widest point, and what appeared to be a loss of continuity in the aortic wall, consistent with rupture, with local blood flow contained by an extensive extraluminal area of heterogeneous echogenicity adjacent to the aortic wall (possibly mural thrombi), forming a pseudoaneurysm. One of the thrombi was impacted in the neck of the pseudoaneurysm, with a small flow identified by color mapping. The tubular ascending aorta presented distal dilatation (55 mm in diameter), while the other aortic segments showed normal flow and diameters. An image suggestive of an intramural hematoma, crescent-shaped and approximately 26 mm deep, was observed on the aortic arch.
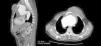
Computed tomography angiography of the thorax (Figure 2) revealed a large aneurysmal lesion involving the ascending thoracic aorta and the aortic arch, measuring approximately 12 mm×93 mm and with significant enlargement of the anterosuperior mediastinum, together with signs of rupture as shown by leakage of its hypodense contents causing cystic swelling of the thorax. It also showed a mural thrombus, 24 mm thick. The aneurysm was causing significant compression of the pulmonary artery trunk, displacing it posteriorly.

During preoperative evaluation, left catheterization and aortography revealed irregularities in the anterior descending and circumflex arteries, with no obstructive lesions, and evidence of an ascending aortic aneurysm compressing the brachiocephalic trunk and left common carotid artery.
Following confirmation of the diagnosis by imaging exams, the patient underwent surgery. Using cardiopulmonary bypass and deep hypothermia, median sternotomy was performed to repair the ruptured aneurysm of the ascending aorta and aortic root with a synthetic vascular graft, with reimplantation and redirection of flow from the brachiocephalic trunk and left carotid artery.
Laboratory tests were requested during the postoperative period to screen for syphilis; nontreponemal (VDRL) and treponemal (chemiluminescent assay) tests were both positive (VDRL 1/64 and chemiluminescent assay 55.74 signal to cut-off ratio).
The clinical course was uneventful, and the patient was discharged within days of surgery. After assessment by an infectologist and negative cerebrospinal fluid test, antibiotic therapy for tertiary syphilis was prescribed.
DiscussionSyphilis is a sexually transmitted disease caused by the bacterium Treponema pallidum. If untreated, it can lead to dermatological, neurological and cardiovascular complications.
The characteristic cardiovascular lesion is aortitis, an inflammatory response to invasion of the aortic wall by spirochetes, which evolves to obliterative endarteritis of the vasa vasorum and results in necrosis of the elastic fibers and connective tissue of the media. The resulting weakening of the aortic wall may progress to the late vascular manifestations of syphilis.1,2
Aortitis, precursor of more serious and symptomatic cardiovascular complications, is reported in 70–80% of untreated cases after the primary infection.3,4
Although now rare, cardiovascular syphilis was demonstrable in 55–86% of cases at autopsy before the discovery of penicillin.5 It was the most common cause of thoracic aortic aneurysm, resulting in 5–10% of cardiovascular deaths.
The ascending aorta is the segment most commonly affected (50%), where it may cause dilatation and aortic valve regurgitation, followed by the arch (35%) and the descending aorta (15%).3
Significant cardiovascular complications occur in 10% of patients,4,6 including aortic aneurysm, aortic regurgitation and coronary ostia stenosis.1,4 The rich lymphatic network in the ascending aorta is believed to be the reason for the greater involvement of this segment.1,7
A pseudoaneurysm is a well-defined collection of blood and connective tissue outside the vessel wall following rupture of the wall. As in left ventricular pseudoaneurysm, aortic pseudoaneurysm is characterized by an extraluminal aneurysmal sac communicating with the true lumen through a relatively narrow neck.2
Clinical manifestations of syphilis typically occur 10–30 years after the initial infection (latent period of the syphilis spirochete) in untreated patients.4 Chest pain is the most common symptom, generally secondary to rapid expansion of an aortic aneurysm, which has a high rate of spontaneous rupture and accounts for up to 80% of deaths within a year of diagnosis unless surgically repaired.8
Aortic rupture is associated with acute onset of excruciating pain, frequently in a region where less intense pain has previously been experienced.2 Surprisingly, our patient reported no episode of acute pain.
Definitive treatment of aortic aneurysms and pseudoaneurysms is surgical repair, which entails resection of the dilated segment of the aorta and implantation of a synthetic vascular graft.6,7
Cardiovascular syphilis can be treated with benzathine penicillin (2.4 million units, intramuscular, once weekly for three weeks), and this was begun in our patient after confirmation of the etiological diagnosis. Patients with symptomatic late syphilis should undergo cerebrospinal fluid testing before therapy is initiated.8,9 Successful antibiotic therapy may halt the progression of aortitis,5 but usually it does not prevent the formation of aortic aneurysms as there is no reversal of post-syphilitic vascular lesions.10
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of dataThe authors declare that no patient data appears in this article.
Right to privacy and informed consentThe authors declare that no patient data appears in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: de Almeida Feitosa IN, Dantas Leite Figueiredo M, de Sousa Belem L, et al. Rara apresentação de aneurisma sifilítico roto de aorta com pseudoaneurisma. Rev Port Cardiol. 2015;34:691.
