



Coronary artery fistula (CAF) is a rare clinical abnormality characterized by a connection between one or more coronary arteries and an adjacent cardiac chamber or vascular structure. Although CAF complications are more common in older children over time, there is still no consensus in terms of treatment indications in children with asymptomatic fistula. We describe an asymptomatic infant diagnosed with a severely dilated right coronary artery and a coronary-cameral fistula treated successfully by transcatheter device closure. The Amplatzer Vascular Plug II appears to be safe, effective and relatively easy to use for CAF closure in infants.
A fístula da artéria coronária (FAC) é uma alteração clínica rara, caracterizada por uma ligação entre uma ou mais artérias coronárias e a câmara cardíaca adjacente ou a estrutura vascular. Embora as complicações da FAC sejam mais comuns em crianças mais velhas, não existe consenso relativamente às indicações da terapêutica em crianças com fístula assintomática. Apresentamos o caso assintomático de uma criança que foi diagnosticada com dilatação grave da artéria coronária direita e fístula coronária-câmara, cujo tratamento foi bem-sucedido através de encerramento por dispositivo percutâneo. Consideramos que o dispositivo Amplatzer Vascular Plig II é seguro, eficaz e de fácil utilização no encerramento da FAC em crianças.
Coronary artery fistula (CAF) is a rare abnormal connection between one or more coronary arteries and an adjacent cardiac chamber or vascular structure. It most commonly affects the right side of the heart1 and occurs in 0.2%–0.4% of cases of congenital heart defect.2 Its size varies from very small presenting with a heart murmur to very large causing heart failure and/or coronary ischemia.3 Angiography is still the preferred method for diagnosis.1 Closure using either a transcatheter approach or surgery is necessary for patients with a symptomatic or hemodynamically significant fistula.1,2 However, there is no consensus with regard to treatment indications in asymptomatic CAF, although complications are more common in older patients.4 We describe an asymptomatic infant diagnosed with a severely dilated right coronary artery (RCA) and a coronary-cameral fistula treated successfully by transcatheter device closure.
Case reportA two-month-old female infant was presented for her routine well-baby examination and was found to have a cardiac murmur. She was clinically well without symptoms or signs of congestive heart failure. She was referred for a cardiac consultation at five months of age. On examination, she had a continuous 3/6 systolic-diastolic murmur. The electrocardiogram showed normal sinus rhythm and possible right ventricular hypertrophy. The echocardiogram showed a markedly dilated right coronary artery (RCA) with continuous flow into the right ventricle (RV) from a coronary fistula draining into the RV. Informed consent was obtained from the parents for cardiac catheterization and occlusion of the CAF under general endotracheal anesthesia. Hemodynamic and saturation data demonstrated a pulmonary to systemic flow ratio of 1.2 with normal resistance indices. RCA and subselective angiography demonstrated a markedly dilated proximal and mid right coronary with contrast draining into the RV under the posterior leaflet of the tricuspid valve (Figure 1A).
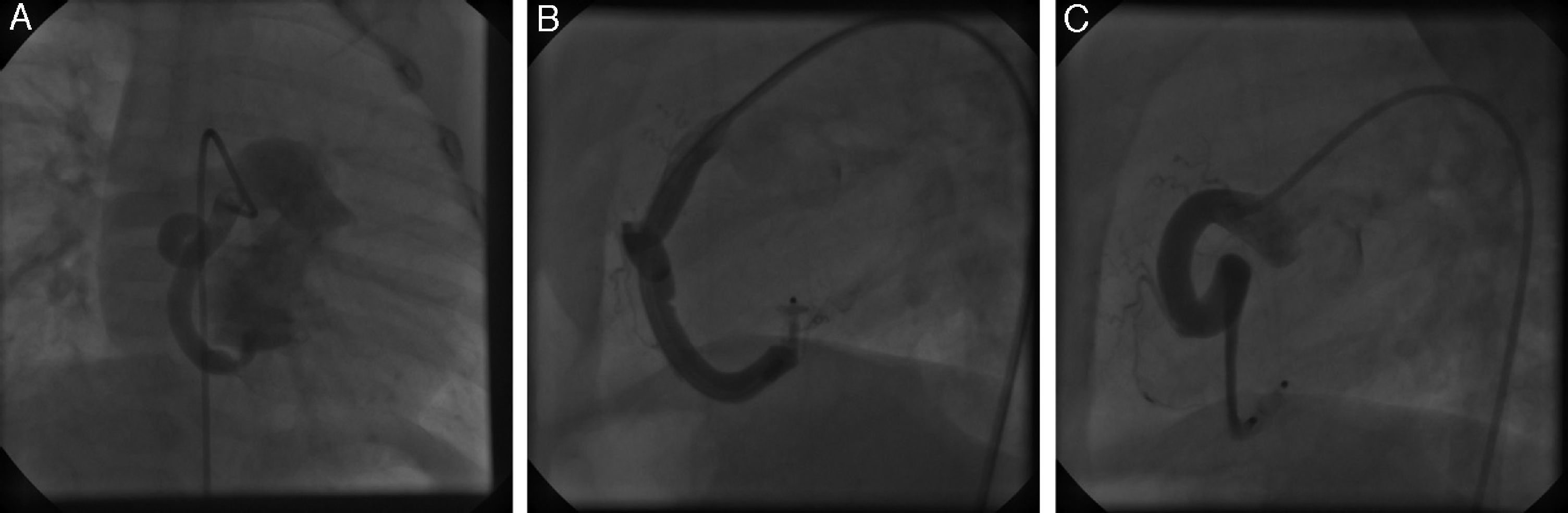
Right coronary artery angiogram in anteroposterior position demonstrating a large right coronary artery fistula draining into the right ventricle just under the posterior leaflet of the tricuspid valve (A); lateral view of the long delivery sheath after deployment and optimal positioning of the Amplatzer vascular plug II device (B); tapering and narrowing in the distal right coronary artery 10 minutes after deployment of the plug (C).
A 4-French (F) angled glide catheter (Terumo Medical, Somerset, NJ) was used retrogradely (via arterial access) to engage the RCA and was advanced distally into the mouth of the fistula. Using a snare with antegrade route (via venous access), an arteriovenous loop was created in the pulmonary artery and was used to advance a 4F long sheath (Cook Medical, Bloomington, IN) deep into the dilated RCA to the level of the fistulous connection with the RV. With the long sheath in position, a 4 mm Amplatzer Vascular Plug II (AVP II) (St. Jude Medical, Austin, TX) was deployed into the mouth of the fistula (Figure 1B). With the plug in position, but not released, a hand injection demonstrated the position of the plug relative to the entry point as well as the location of the normal right coronary branches. One recapture and readjustment of the plug was required to optimize the location and to ensure patency of the main RCA and its branches. The plug was then released, the sheath withdrawn from the RCA, and another angiogram 10 minutes after deployment of the plug demonstrated successful complete occlusion of the fistula as well as some vasospasm in the distal segment of the dilated RCA, with tapering and narrowing (Figure 1C). Nitroglycerin was administered with some mild improvement in the distal vessel and no compromise of flow in the normal coronary branches. There was no cardiac murmur, continuous flow on echocardiography or ST-T wave changes indicating ischemia, and the RV remained normal over 24 hours post-procedure. The patient was discharged home on once daily aspirin therapy planned for six months.
DiscussionAlthough there are several reports of spontaneous closure of CAF, percutaneous interventional treatment is the preferred approach for large fistulas due to their potential complications such as pulmonary hypertension, heart failure, endocarditis, rupture, thrombosis, and myocardial ischemia. CAF may become more complicated with age, as suggested by some previous reports.4–6
The vascular plug device we used is characterized by a close-knit 144-wire nitinol mesh with no fabric, allowing the device to be delivered through a smaller delivery catheter with diameter up to 22 mm. The device is user-friendly and attached to a flexible delivery cable. A single plug is usually effective for closure without the use of additional devices.7,8 Although cost comparisons may favor coils, the fact that only a single AVP II is commonly needed, and the reduced need to maintain catheter position during multiple coil deployments, make it advantageous for occluding larger vascular structures.7 Additionally, deployment of several coils results in increased fluoroscopy time, contrast volume, and costs, as well as a risk of embolization due to high flow in arterial vessels, often favoring the vascular plug device. In our case, a retrograde route (via arterial access) was chosen due to the anatomic location of the entry point of the CAF and the inability to stabilize a delivery sheath in an optimal position from a transvenous approach. Also, attempting this procedure using an antegrade approach can increase the risk of tricuspid valve damage.9 Clearly there are trade-offs as the retrograde approach can result in damage to the RCA and thrombotic coronary complications. Minimizing catheter dwell time within the coronary artery, efficient workflow, and optimizing anticoagulation regimens are keys to success when taking this approach. Since we were able to perform multiple hand-injection angiographies via the side arm of a Tuohy-Borst connection for evaluation of the blood flow of small RCA branches, we did not use balloon test occlusion during the procedure.
Gonçalves et al.10 from Portugal presented an 11-year-old boy diagnosed with a large CAF and transcatheter closure via arterial access using both an AVP II and an Amplatzer duct occluder (AGA Medical Corporation, Golden Valley, MN). Jang et al.11 from South Korea and Balaguru et al.3 from Boston reported successful transvenous closure of a large CAF with a single AVP in three-year-old and two-year-old females, respectively. Ismail et al.4 from the UK performed transcatheter occlusion of a CAF using an AVP II in an 11-month-old boy. To the best of our knowledge, our patient is the youngest case in the literature to undergo percutaneous closure of a CAF with an AVP II via a retrograde approach.
In conclusion, the Amplatzer Vascular Plug II appeared safe, effective and relatively easy to use for CAF closure in this infant. Larger studies and even randomized trials comparing this approach to surgery would be valuable.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interestThe authors have no conflicts of interest to declare.
