






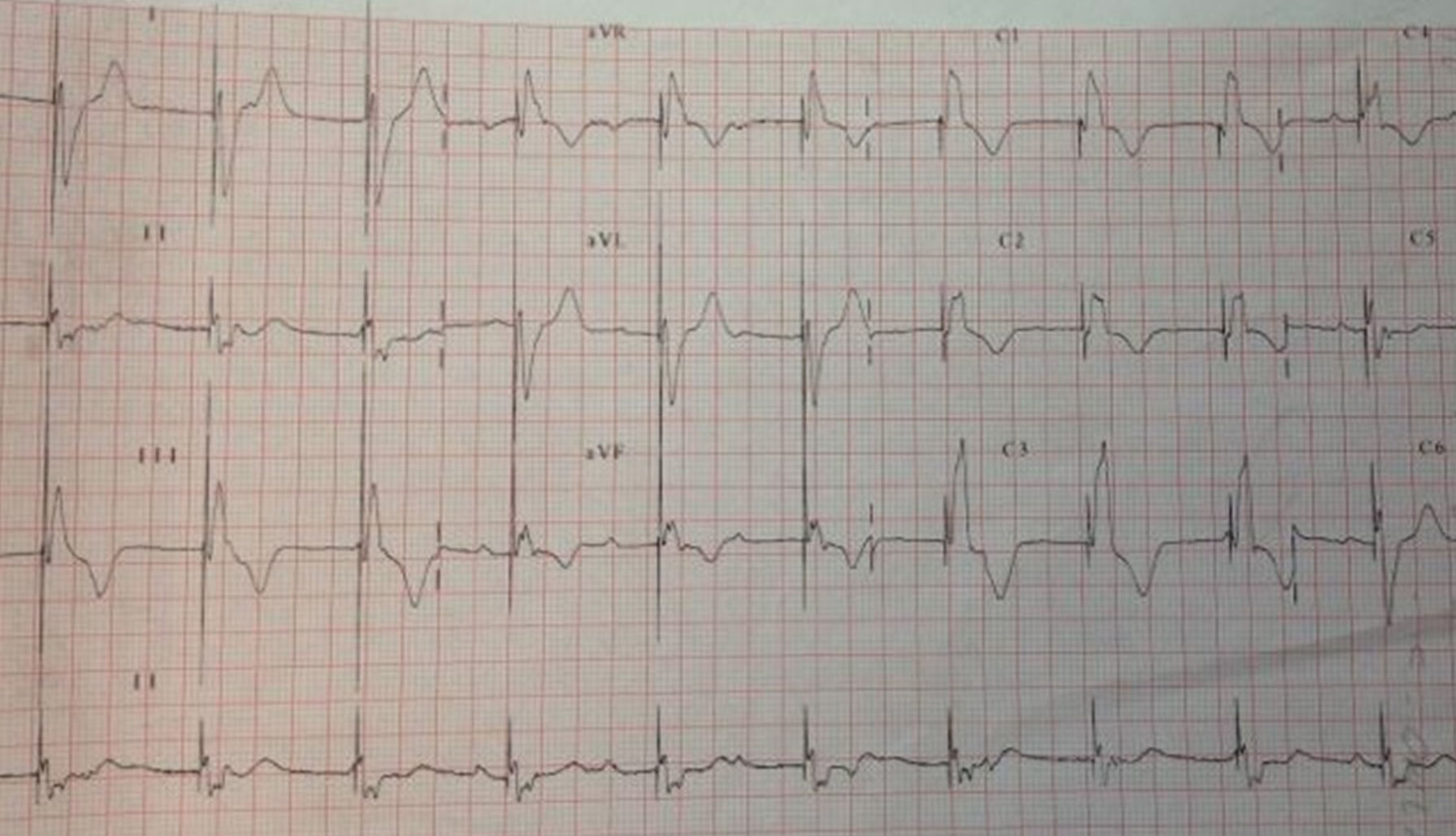
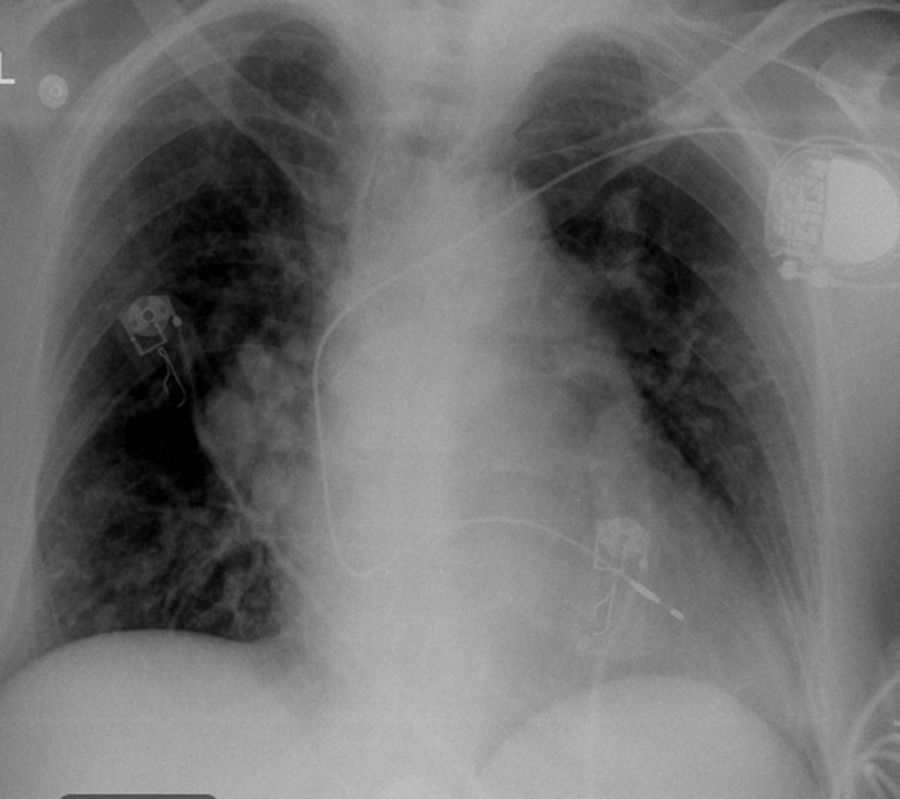
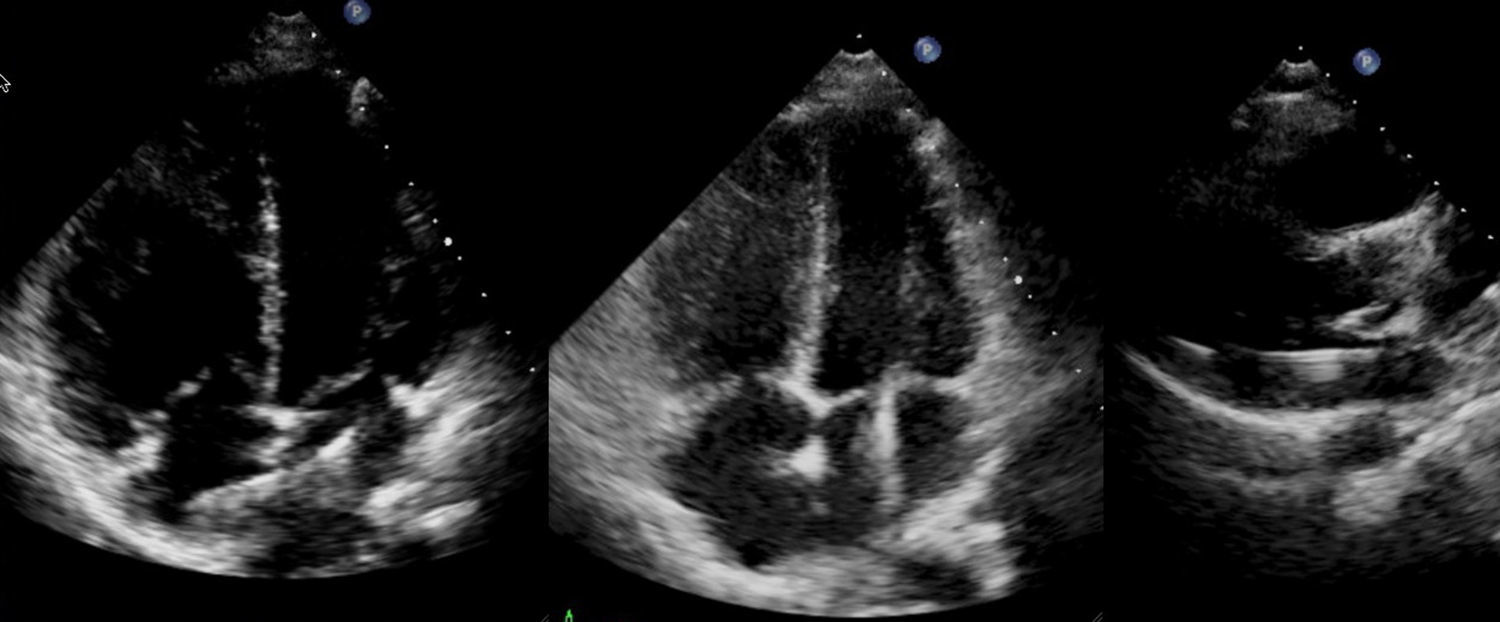
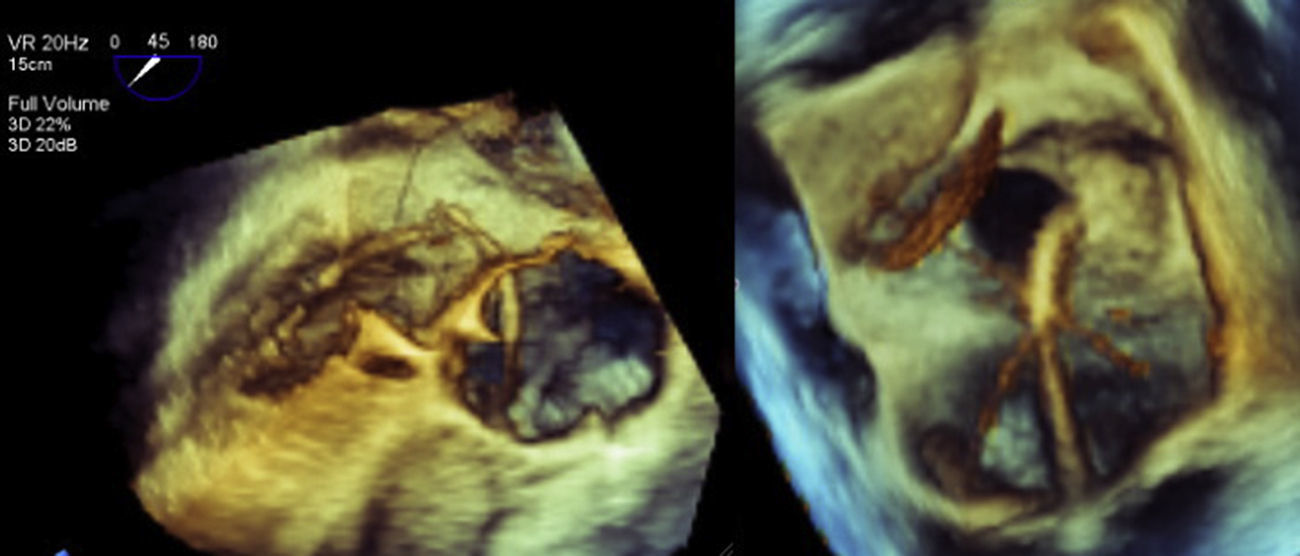
A 70-year-old woman with a permanent VVI pacemaker implanted two years previously for advanced atrioventricular block came to our emergency department due to chest pain, dyspnea and palpitations for the past two hours. An electrocardiogram performed at that time showed atrial fibrillation at 140 bpm. After electrical cardioversion, the electrocardiogram during ventricular pacing showed a right bundle branch block pattern (Figure 1). No chest X-ray was performed at that time, but a previous one was investigated (Figure 2). A transthoracic echocardiogram (Figure 3) suggested malposition of the pacemaker lead in the left ventricle with right atrial and ventricular dilatation, so a three-dimensional transesophageal echocardiogram (Figure 4) was obtained that showed the pacemaker lead passing through a 2-cm interatrial communication and the mitral valve, and finally into the left ventricle.
Pacemaker lead malposition in the left ventricle is an uncommon complication but probably underdiagnosed due to its asymptomatic character in most cases.
This complication should be considered when right bundle branch block is seen on a pacing electrocardiogram and the pacemaker lead has a posterior position on the lateral chest X-ray. A definitive diagnosis is obtained by echocardiography.
In asymptomatic patients, long-term anticoagulation therapy is preferred but in this case, with a symptomatic interatrial communication, we decided on surgical retraction of the lead and permanent closure of the septal defect.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
