


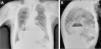
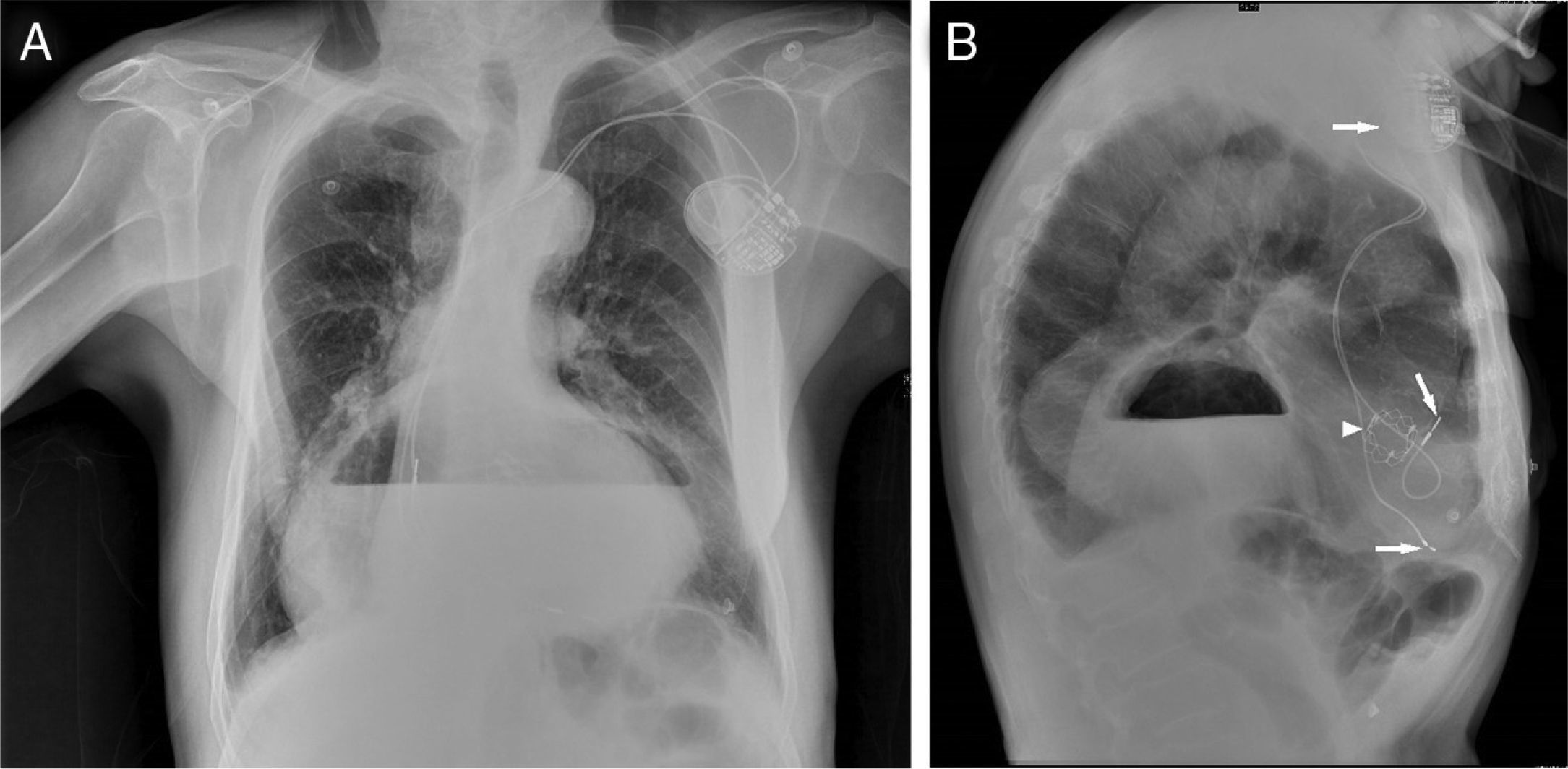
An 89-year-old man presented with intermittent chest and epigastric pain, nausea and vomiting of one day's duration. His previous medical history included coronary artery disease and severe aortic valve stenosis, treated by transcatheter aortic valve implantation (26 mm Edwards®) 14 months before. After the procedure, he suffered complete atrioventricular block, and a dual chamber pacemaker was implanted. Physical examination revealed low-grade fever (37.6°C) and an aortic systolic murmur; no pain was elicited on thoracic or abdominal examination. Laboratory findings included high-sensitivity cardiac troponin 0.073 ng/ml (normal 0.003–0.014), myoglobin 153 ng/ml (normal 28–72) and C-reactive protein 4.5 mg/dl (normal <0.5). The electrocardiogram showed ventricular pacing and transthoracic echocardiography revealed no significant abnormal findings. The chest X-ray (posteroanterior view) showed widening of the mediastinum, with air-fluid level at the level of the cardiac silhouette (Figure 1A). In lateral view (Figure 1B), the air-fluid level was located behind the heart. Both pacemaker generator and leads (arrows) and biological aortic valve (arrowhead) are seen in this view. Upper gastrointestinal endoscopy confirmed a type III paraesophageal hiatus hernia, with signs of mucosal ischemia. Urgent surgical correction (Dor fundoplication) was performed. The postoperative period was complicated by respiratory and surgical wound infections. The patient was discharged to a rehabilitation unit 65 days after admission.
We report the case of a man who presented with a life-threatening condition, diagnosed with a chest X-ray. In this era of ultra-high technology, sometimes clinical history, physical examination and simple and inexpensive exams provide the diagnosis.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
