




Intravenous leiomyomatosis is an unusual clinical condition characterized by histologically benign smooth muscle lesions extending from the uterus into pelvic and systemic veins and, more rarely, into the right cardiac chambers. We report the case of a 45-year-old woman who presented with a three-week history of dyspnea on exertion, shortness of breath and fatigue. Echocardiography showed a large mobile mass in the right atrium prolapsing into the right ventricle and extending to the inferior vena cava. A computed tomography scan revealed a large mass extending from the right atrium to the inferior vena cava and through the systemic veins as far as the popliteal veins. A presumptive diagnosis of large thrombus was made; the correct diagnosis of intravenous leiomyomatosis with intracardiac involvement was obtained only after surgical resection and histologic examination.
A Leiomiomatose intravascular é uma situação clínica invulgar caracterizada histologicamente por lesões benignas de tecido muscular liso que se estendem a partir do útero para as veias pélvicas e suas aferentes, raramente atingindo as cavidades cardíacas direitas. Descrevemos o caso de uma mulher de 45 anos que se apresentou com dispneia de esforço, polipneia e fadiga, com três semanas de evolução. O ecocardiograma mostrou uma massa grande e móvel no interior da aurícula direita, com prolapso para o ventrículo direito e extensão para a veia cava inferior. A tomografia computorizada revelou uma massa que se estendia da aurícula direita para a veia cava inferior e ao longo das veias sistémicas até às veias popliteias. Foi feito o diagnóstico presuntivo de trombo extenso; o diagnóstico correto de leiomiomatose intravascular com envolvimento intra-cardíaco só foi possível após ressecção cirúrgica e exame histológico.
Intracardiac masses can be classified in three basic types: tumors (rarely primary tumors such as myxoma, lipoma or sarcoma; more often cardiac metastases from melanoma or lung, breast, ovarian or kidney cancer), thrombus, or vegetation. A reasonably secure diagnosis can often be made by integrating clinical data with the echocardiographic appearance.1 A specific type of cardiac involvement by tumor is that of uterine tumors in which a finger-like projection may protrude into the right atrium (RA) from the inferior vena cava (IVC). This situation is called intravenous leiomyomatosis (IVL).
Case reportA 45-year-old nulliparous Caucasian woman was admitted to our hospital with a three-week history of dyspnea on exertion, shortness of breath and fatigue. She had a medical history of ankylosing spondylitis, multiple sclerosis and a benign subserous uterine leiomyoma (diagnosed in 1997, not treated surgically).
No notable changes were identified on physical examination and her vital signs were stable. The electrocardiogram showed sinus tachycardia and the chest radiography was normal. Arterial blood gases, serum troponin levels, and hematologic and coagulation parameters were within the normal range.
Transthoracic echocardiography showed a large mobile mass within the RA prolapsing into the right ventricle during diastole; left and right ventricular systolic function was preserved. Transesophageal echocardiography showed the mass extending from the IVC through the RA and crossing the tricuspid valve into the right ventricle during diastole; no adherences to cardiac walls or valves were detected (Figure 1).
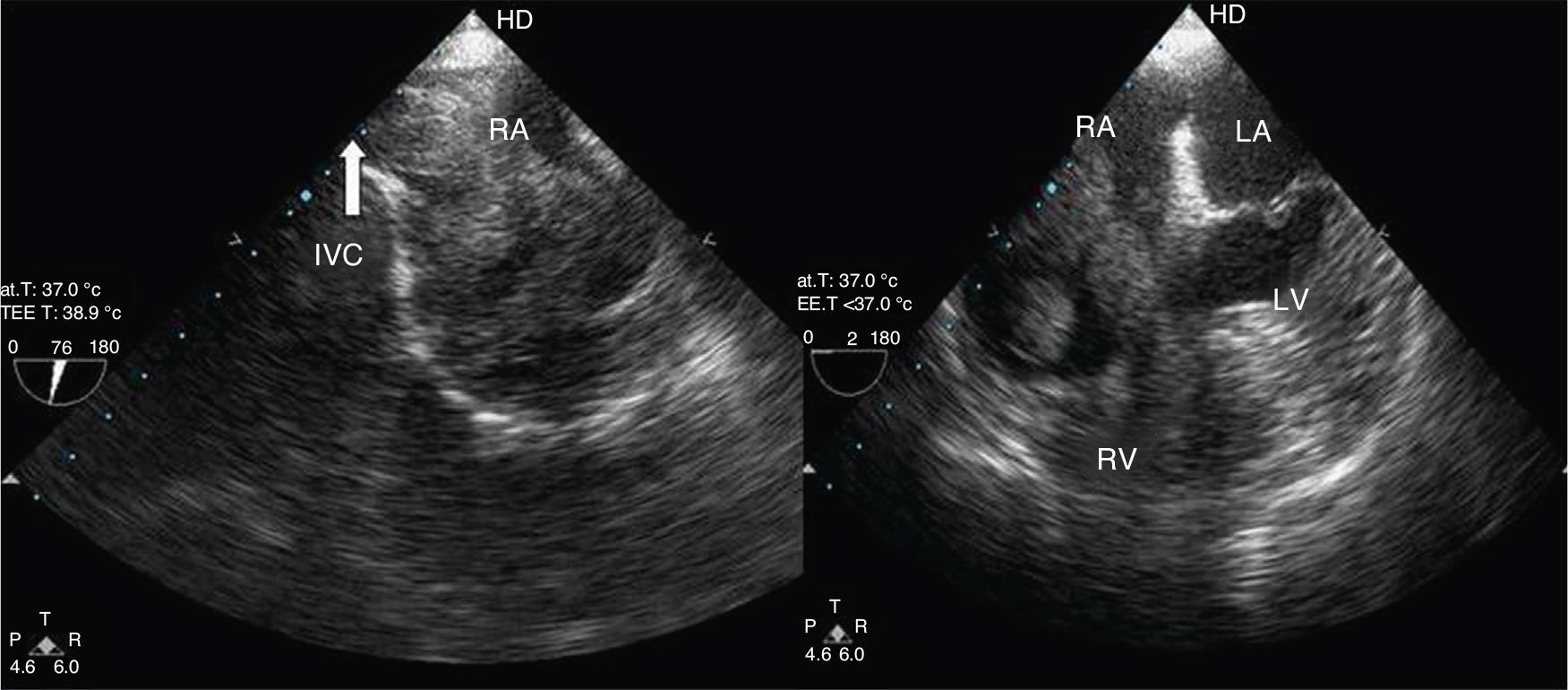
Transesophageal echocardiography. Bicaval (left) and 4-chamber view (right) showing an elongated mass extending from the inferior vena cava through the right atrium and crossing the tricuspid valve into the right ventricle. IVC: inferior vena cava; LA: left atrium; LV: left ventricle; RA: right atrium; RV: right ventricle.
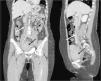
An enhanced chest, abdominal and pelvic computed tomography (CT) scan showed a thrombus-like filling defect image extending from the RA as far as the popliteal veins, involving the IVC and bilateral iliac and femoral veins (Figure 2). Uterine fibroids were present and pulmonary embolism was excluded.

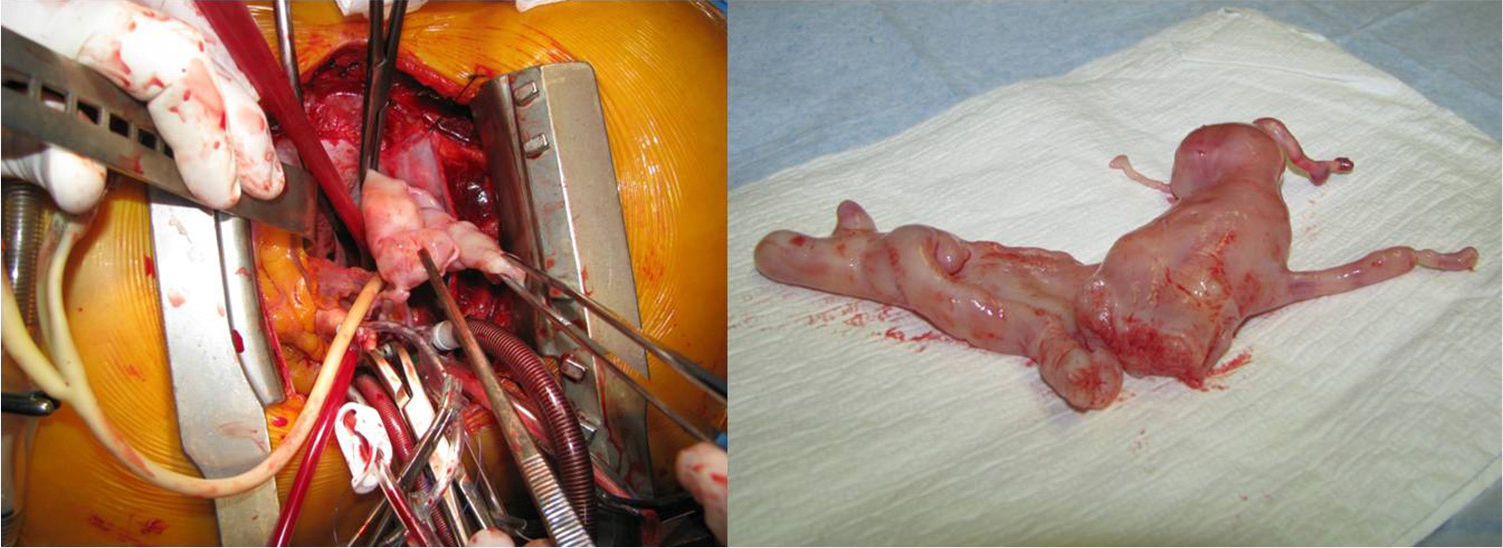
A presumptive diagnosis of large thrombus was made and the patient was started on unfractionated heparin therapy. The cardiothoracic surgery center was consulted and the patient was referred for emergency surgery. Primary median sternotomy was performed, as was cardiopulmonary bypass from the superior vena cava to the ascending aorta. Following right atriotomy, a large vermiform tumor was found occupying most of the RA and extending into the IVC; the mass was free-floating without invasion, and so it was pulled outward as far as possible and then sectioned (Figure 3).
Pathologic examination of the specimen showed leiomyomatous tissue. A control CT scan showed a tumoral mass within the primitive iliac veins and IVC up to the confluence of the renal veins.
The postoperative course was uneventful and the patient was discharged seven days after surgery. She was proposed for a second stage of the procedure, in which excision of the remaining tumor would be performed as well as total hysterectomy with bilateral salpingo-oophorectomy, but she refused.
DiscussionIVL is a unusual benign smooth-muscle cell tumor, which develops in the uterus and grows in a worm-like fashion into pelvic and systemic veins.2,3 Although histologically benign, IVL has metastatic potential due to intravascular spread. The tumor is usually confined to the pelvic venous system, but can progress along the veins into the IVC in 10% of cases, and rarely into the right side of the heart (3%).4 The lesions of IVL were first described by Birch-Hirschfield in 1897, and in 1907 Durck reported the first case of intracardiac extension.5,6
There are two main theories regarding the origin and growth mechanism of IVL: intravenous projections of an uterine leiomyoma, or direct carcinogenesis from the vascular walls within the myometrium.3,7 The tumor can be entirely free-floating within the vessel lumen or, less commonly, can have attachments to vessel or atrial walls.
The disease generally occurs in middle-aged women, most of whom have coexisting uterine leiomyoma, like our patient, or a history of hysterectomy. There has been no proven correlation with race, fertility or parity.2,8
Women may experience pelvic, abdominal or cardiac symptoms, depending on the extent of the mass. Our patient had no symptoms associated with the uterine leiomyoma; her complaints were related to intracardiac involvement. According to Wu et al., the most common presentation is heart failure.9 The development of collateral vessels may be one explanation for the fact that even patients with extensive intravascular masses and IVC occlusion may remain asymptomatic until direct intracardiac growth causes heart failure. Serious complications, like syncopal episodes, cardiogenic shock, pulmonary embolism or even sudden cardiac death, have also been reported.3,4,9
Several imaging studies may help establish the diagnosis. Intracardiac masses can be assessed by echocardiography; computed tomography (CT) and magnetic resonance (MR) imaging can provide additional information on the extension of the lesion and can also detect associated uterine leiomyoma or pulmonary emboli.10
Two-dimensional echocardiography usually shows an elongated mobile mass, the most important echocardiographic feature being the penetration of the tumor from the abdominal venous system into the RA.9,11–13 Transesophageal echocardiography provides better spatial resolution and information about where the tumor is attached to the atrial wall or interatrial septum and the relationship with the IVC and superior vena cava.9,12
However, accurate preoperative diagnosis of IVL is still usually difficult.7,14 In the present case, a precise diagnosis was not obtained before surgical resection and histologic examination because the initial presentation and findings pointed to a large thrombus. In fact, mainly because of its rarity, cases of intracardiac leiomyomatosis may be misdiagnosed as primary cardiac tumor, venous thrombus-in-transit or, occasionally, as renal cell carcinoma or hepatoma, which may also extend into the right cardiac chambers via the IVC.11–13,15 The characteristics and attachment site of the tumor detected by echocardiography may offer important information for the differential diagnosis of a right atrial mass.12
Surgery remains the gold standard treatment; complete removal of the tumor, with hysterectomy and resection of all extra-uterine masses, is mandatory for a favorable outcome and to avoid recurrence.3,4,7–9,16 The first successful resection of intracardiac extension of such tumors was reported by Timmis et al. in 1980.17
Surgery can be performed in two stages – resection of the intrathoracic tumor and of the abdominal/pelvic tumor in two separate operations – or, more recently, through a one-stage operation, involving total resection of the tumor.18,19 Many authors still consider the two-stage procedure to be safer and easier.4,7,17 The slow growth of the tumor allows for a safe interval between the two surgeries.4 Bilateral oophorectomy is also considered essential, because the tumor is estrogen-dependent.9,16 For the same reason, anti-hormone therapy should be considered in cases of unresectable residual tumor, although its efficacy is still controversial.4,16
If the tricuspid valve has been destroyed by the tumor, tricuspid valvuloplasty or valve replacement should be carried out.12,13
Long-term prognosis of IVL is usually good if the tumor can be completely removed. However recurrence and metastases are not unusual and can be found up to 15 years after surgery. Long-term follow-up is therefore recommended, including thorax and abdomen CT scan and serial echocardiography.3,10,13,15 Reintervention is recommended in cases of recurrence to achieve long-term disease-free survival.4,12
ConclusionsIVL should be suspected on detection of a right atrial mass originating from the IVC in a middle-aged woman, especially with a history of uterine fibroids or hysterectomy. Imaging studies are helpful in the diagnosis. Successful therapy is mainly dependent on total surgical resection.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interestThe authors have no conflicts of interest to declare.
