

Cardiorenal syndrome (CRS) is common in acute heart failure (AHF), and is associated with dire prognosis. Levosimendan, a positive inotrope that also has diuretic effects, may improve patients’ renal profile. Published results are conflicting.
ObjectivesWe aimed to assess the incidence of CRS in AHF patients according to the inotrope used and to determine its predictors in order to identify patients who could benefit from the most renoprotective inotrope.
MethodsIn a retrospective study, 108 consecutive patients with AHF who required inotropes were divided into two groups according to the inotrope used (levosimendan vs. dobutamine). The primary endpoint was CRS incidence. Follow-up for mortality and readmission for AHF was conducted.
ResultsSeventy-one percent of the study population were treated with levosimendan and the remainder with dobutamine. No differences were found in heart failure etiology or chronic kidney disease. At admission, the dobutamine group had lower blood pressure; there were no differences in estimated glomerular filtration rate or cystatin C levels. The levosimendan group had lower left ventricular ejection fraction. CRS incidence was higher in the dobutamine group, and they more often had incomplete recovery of renal function at discharge. In multivariate analysis, cystatin C levels predicted CRS. The dobutamine group had higher in-hospital mortality, of which CRS and the inotrope used were predictors.
ConclusionsLevosimendan appears to have some renoprotective effect, as it was associated with a lower incidence of CRS and better recovery of renal function at discharge. Identification of patients at increased risk of renal dysfunction by assessing cystatin C may enable more tailored therapy, minimizing the incidence of CRS and its negative impact on outcome in AHF.
A síndrome cardiorrenal (SCR) é comum na insuficiência cardíaca aguda (ICA), associando-se a um prognóstico sombrio. O levosimendano, aliando um efeito inotrópico e diurético, poderá ter melhor perfil renal. A literatura é controversa.
ObjetivosAvaliar em doentes com ICA a incidência de SCR em função do inotrópico utilizado. Determinar preditores de SCR, identificando os doentes que possam beneficiar do inotrópico com melhor perfil renoprotetor.
MétodosEstudo retrospetivo, incluindo 108 doentes consecutivos com ICA tratados com inotrópicos. Criados dois grupos consoante o inotrópico utilizado (levosimendano e dobutamina). O endpoint primário foi incidência de SCR. Realizado seguimento relativo a mortalidade e hospitalização por ICA.
ResultadosO levosimendano foi usado em 71% dos doentes e a dobutamina nos restantes. Sem diferenças na etiologia da IC ou incidência de doença renal crónica. À admissão, o grupo-dobutamina apresentava menor pressão arterial sistólica; sem diferenças na taxa de filtração glomerular (TFG) ou cistatina C. O grupo-levosimendano apresentava disfunção ventricular esquerda mais grave. A incidência de SCR foi maior no grupo-dobutamina, com recuperação incompleta da TFG à alta hospitalar. Em análise multivariada, a cistatina C foi preditora de SCR. A mortalidade intra-hospitalar foi superior no grupo-dobutamina, sendo a SCR e o inotrópico utilizado preditores desta.
ConclusõesO levosimendano parece ter melhor perfil renal, associando-se a menor incidência de SCR, com recuperação da função renal. A cistatina C, ao identificar os doentes em maior risco de disfunção renal, poderá permitir uma terapêutica mais individualizada, reduzindo a incidência de SCR e seu impacto negativo no prognóstico da ICA.
Acute heart failure (AHF) remains the single most common admitting diagnosis in industrialized countries, despite significant advances in pharmacologic and device therapy.1,2 Some degree of renal impairment is present in more than a third of patients with AHF, associated with reduction in renal blood flow and/or elevation in central venous pressure, leading to a decrease in estimated glomerular filtration rate (eGFR).3–5 Conversely, renal impairment itself may predispose to worsening heart failure (HF), through constant salt and water retention, diuretic resistance and neurohormonal activation, leading to increased cardiac workload.6,7 In a broad spectrum of patients with chronic HF in the CHARM study,8 renal dysfunction was independently associated with increased risk of death, cardiovascular death, and hospitalization due to AHF.9 Furthermore, in advanced chronic HF, renal impairment was a stronger predictor of mortality than either left ventricular ejection fraction (LVEF) or New York Heart Association (NYHA) functional class.10
Both dobutamine and levosimendan are inotropic drugs, used specifically to improve cardiac contractility.11 Through activation of ATP-sensitive potassium channels, levosimendan causes both arterial and venous vasodilation (mainly the latter).11 This additional effect of levosimendan over dobutamine may be crucial in AHF, since central venous pressure is an independent predictor of cardiorenal syndrome (CRS) in this setting.12
However, only a few studies comparing the effects of levosimendan with dobutamine on renal function in patients hospitalized with AHF have been published.13,14
We aimed to assess the incidence of CRS according to the inotrope used and to determine its predictors in order to identify patients who could benefit from the most renoprotective inotrope.
The primary endpoint was CRS incidence during hospital stay. The secondary endpoints were recovery of eGFR at discharge, readmission for AHF and mortality during follow-up.
MethodsPopulation and study designWe retrospectively studied 108 consecutive patients admitted between May 2009 and March 2014 to a single cardiac intensive care unit for AHF with symptoms or signs of severe congestion or low cardiac output requiring inotropes. The diagnosis of AHF was established according to the current European Society of Cardiology guidelines.15
Patients with end-stage renal disease on a regular program of renal replacement therapy were excluded.
The sample was divided into two groups according to the inotrope used (levosimendan or dobutamine), prescribed at the discretion of the admitting physician. In the levosimendan group no initial bolus was given and perfusion was started at 0.1 μg/kg/min and titrated up to 0.2 μg/kg/min if tolerated. In the dobutamine group perfusion was started at 5.0 μg/kg/min and titrated on a clinical basis.
CRS was defined as an increase of ≥26.5 μmol/l in serum creatinine relative to the admission value.16 The Modification of Diet in Renal Disease (MDRD) equation was used to calculate eGFR, according to the recommendations of the KDIGO Clinical Practice Guideline for Acute Kidney Injury.17 Changes in renal function were assessed by determining maximum and discharge creatinine and blood urea nitrogen (BUN) and minimum eGFR.
The study is in accordance with the principles outlined in the Declaration of Helsinki.
Data collectionBaseline data were collected from patients’ medical records and included previous medical history (time course and etiology of HF, ischemic heart disease, hypertension, diabetes and chronic renal failure and current therapy), physical examination at admission (heart rate and blood pressure), electrocardiogram and blood test analysis (creatinine, BUN, ionogram, N-terminal pro-B-type natriuretic peptide [NT-pro-BNP], hemoglobin, total bilirubin, alkaline phosphatase, aspartate transaminase [AST], alanine transaminase [ALT] and cystatin C).
All patients underwent transthoracic echocardiography with assessment of both systolic (LVEF by the modified Simpson's rule) and diastolic function.
Therapies analyzed were maximum daily dose of furosemide and type of administration (bolus vs. perfusion), use of vasodilator doses of dopamine and noradrenaline, renal support therapy and noninvasive or invasive mechanical ventilation.
In-hospital mortality and length of hospital stay were analyzed.
Readmission for AHF and mortality during follow-up were also obtained from clinical records from outpatient clinic, hospital ward and emergency department admissions and through phone calls for patients not followed at our hospital.
Statistical analysisThe statistical analysis was performed with SPSS version 21.0 (IBM SPSS Inc., Chicago, IL, USA).
Data were summarized using means, standard errors, numbers and percentages, as appropriate. The chi-square test was used for dichotomous variables and the independent-samples t test for continuous variables with normal distribution. Multivariate analysis was used to determine predictors of CRS and in-hospital mortality. Statistical significance was defined as p<0.05.
ResultsPatient characteristicsOne hundred and eight consecutive patients admitted to our cardiac intensive care unit with AHF were studied. Mean age was 66±15 years and 74% were male. According to the decision of the admitting physician, 77 patients (71%) were treated with levosimendan and the remaining 31 (29%) with dobutamine.
Comparison of baseline characteristics and therapeutic strategiesPatients in the levosimendan group were younger and more frequently male.
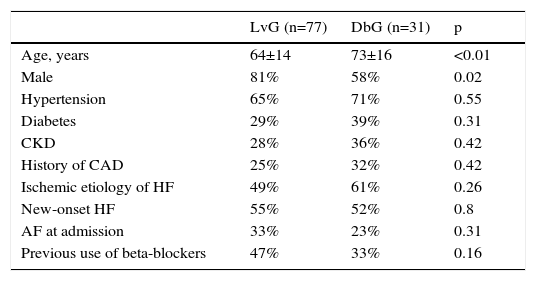
No differences were found between the groups in HF etiology (ischemic vs. non-ischemic) or previous history of coronary artery disease, hypertension, diabetes or chronic kidney disease. In both groups, the incidence of new-onset HF was similar. The most frequent precipitating factor (acute coronary syndrome: 35% vs. 55%, p=0.06) was similar in both groups, as were atrial fibrillation incidence at admission and previous use of beta-blockers. Table 1 presents the details of the above data.
Comparison of patient characteristics at baseline.
| LvG (n=77) | DbG (n=31) | p | |
|---|---|---|---|
| Age, years | 64±14 | 73±16 | <0.01 |
| Male | 81% | 58% | 0.02 |
| Hypertension | 65% | 71% | 0.55 |
| Diabetes | 29% | 39% | 0.31 |
| CKD | 28% | 36% | 0.42 |
| History of CAD | 25% | 32% | 0.42 |
| Ischemic etiology of HF | 49% | 61% | 0.26 |
| New-onset HF | 55% | 52% | 0.8 |
| AF at admission | 33% | 23% | 0.31 |
| Previous use of beta-blockers | 47% | 33% | 0.16 |
AF: atrial fibrillation; CAD: coronary artery disease; CKD: chronic kidney disease; DbG: dobutamine group; HF: heart failure; LvG: levosimendan group.
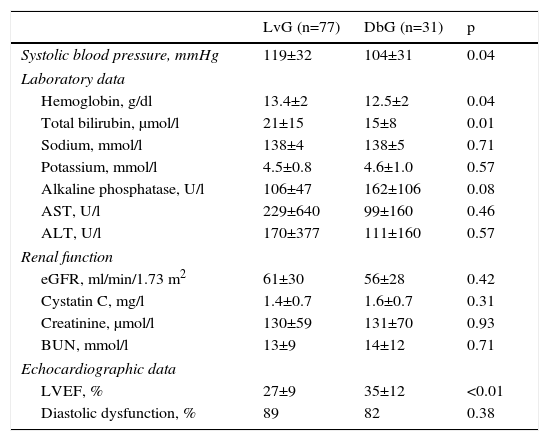
Table 2 summarizes the main clinical, laboratory and echocardiographic data at admission. Systolic blood pressure and hemoglobin were lower in the dobutamine group and total bilirubin was higher in the levosimendan group, but there were no differences in sodium, potassium, alkaline phosphatase, AST or ALT. LVEF was lower in the levosimendan group, with no differences between groups regarding prevalence of diastolic dysfunction.
Main clinical, laboratory and echocardiographic data.
| LvG (n=77) | DbG (n=31) | p | |
|---|---|---|---|
| Systolic blood pressure, mmHg | 119±32 | 104±31 | 0.04 |
| Laboratory data | |||
| Hemoglobin, g/dl | 13.4±2 | 12.5±2 | 0.04 |
| Total bilirubin, μmol/l | 21±15 | 15±8 | 0.01 |
| Sodium, mmol/l | 138±4 | 138±5 | 0.71 |
| Potassium, mmol/l | 4.5±0.8 | 4.6±1.0 | 0.57 |
| Alkaline phosphatase, U/l | 106±47 | 162±106 | 0.08 |
| AST, U/l | 229±640 | 99±160 | 0.46 |
| ALT, U/l | 170±377 | 111±160 | 0.57 |
| Renal function | |||
| eGFR, ml/min/1.73 m2 | 61±30 | 56±28 | 0.42 |
| Cystatin C, mg/l | 1.4±0.7 | 1.6±0.7 | 0.31 |
| Creatinine, μmol/l | 130±59 | 131±70 | 0.93 |
| BUN, mmol/l | 13±9 | 14±12 | 0.71 |
| Echocardiographic data | |||
| LVEF, % | 27±9 | 35±12 | <0.01 |
| Diastolic dysfunction, % | 89 | 82 | 0.38 |
ALT: alanine transaminase; AST: aspartate transaminase; BUN: blood urea nitrogen; DbG: dobutamine group; eGFR: estimated glomerular filtration rate; HF: heart failure; LVEF: left ventricular ejection fraction; LvG: levosimendan group.
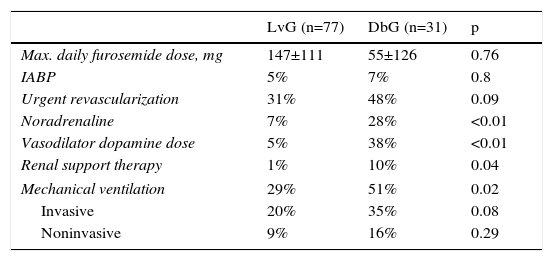
Table 3 shows the main differences in treatment between the groups. There were no differences in maximum daily dose of furosemide or its form of administration (bolus vs. infusion). The use of intra-aortic balloon-pump counterpulsation and urgent revascularization was similar between groups. Noradrenaline and dopamine in vasodilator doses were more frequent in the dobutamine group, as was the need for renal support therapy and mechanical ventilation.
Main differences in therapeutic strategies between the study groups.
| LvG (n=77) | DbG (n=31) | p | |
|---|---|---|---|
| Max. daily furosemide dose, mg | 147±111 | 55±126 | 0.76 |
| IABP | 5% | 7% | 0.8 |
| Urgent revascularization | 31% | 48% | 0.09 |
| Noradrenaline | 7% | 28% | <0.01 |
| Vasodilator dopamine dose | 5% | 38% | <0.01 |
| Renal support therapy | 1% | 10% | 0.04 |
| Mechanical ventilation | 29% | 51% | 0.02 |
| Invasive | 20% | 35% | 0.08 |
| Noninvasive | 9% | 16% | 0.29 |
DbG: dobutamine group; IABP: intra-aortic balloon-pump counterpulsation; LvG: levosimendan group; Max.: maximum.
The dobutamine group had a higher incidence of the primary endpoint of CRS (49% vs. 77%, p<0.01) and lower minimum eGFR (44±22 vs. 31±18 ml/min/1.73 m2, p<0.01).
Furthermore, the percentage of decrease in eGFR during hospital stay was higher in the dobutamine group than in the levosimendan group (24±21% vs. 38±28%, p=0.02).
At discharge, patients who received dobutamine presented a trend towards partial recovery in renal function (eGFR 56±28 ml/min/1.73 m2 at admission vs. 45±25 ml/min/1.73 m2 at discharge, p=0.06), unlike patients treated with levosimendan (eGFR 61±30 ml/min/1.73 m2 at admission vs. 60±27 ml/min/1.73 m2 at discharge, p=0.67).
Changes in renal function parameters are represented in Figure 1.

Using logistic regression analysis, which included all variables that differed between the groups, cystatin C (odds ratio [OR] 8.6, 95% confidence interval [CI] 1.8-40.7, p=0.007) was identified as the only predictor for CRS development during hospital stay (p=0.73 for the Hosmer-Lemeshow test).
In-hospital prognosisLength of stay was similar in both groups (10±8 vs. 12±9 days, p=0.29). In-hospital mortality (19%) was higher in the dobutamine group (9% vs. 42%, p<0.01). CRS (OR 13, 95% CI 1.5-114.4, p=0.02) and the inotrope used (OR for dobutamine 5, 95% CI 1.47-19.92, p=0.01) were independent predictors of mortality.
Follow-upDuring follow-up (481±365 days), 44 patients were readmitted due to AHF and 39 died. There were no differences between the groups regarding mortality (41% vs. 56%, p=0.28), readmission due to AHF (47% vs. 61%, p=0.29), or the composite endpoint of death and readmission due to AHF (64% vs. 67%, p=0.85).
DiscussionRenal dysfunction is one of the most important and prevalent comorbidities of HF and has emerged as a critical risk factor for prolonged hospitalization and rehospitalization and short- and long-term mortality in patients with AHF.18 The prevalence of CRS in our study was very high in both groups (49% and 77%) (although similar to that reported in a sub-analysis of the ADHERE database4), and was an independent predictor of mortality, associated with a risk of death thirteen times higher than in those who did not develop CRS. The high prevalence of acute kidney injury might be explained by the characteristics of our study population, since we only included patients who required treatment with inotropes, which is a surrogate marker of low cardiac output. Factors such as age (mainly elderly) and high incidences of hypertension, diabetes and coronary artery disease, all of them recognized contributors to renal dysfunction, may also have had an impact.4
Unfortunately, the clinical management of CRS is largely empirical and many drugs traditionally used to treat HF (diuretics, angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, and aldosterone antagonists) may result in renal dysfunction due to their serious side effects, especially following inappropriate or excessive use.19,20
Levosimendan is a positive inotropic drug with vasodilatory properties that has been assessed in several clinical studies in patients with AHF, which demonstrated improvements in renal hemodynamics and laboratory markers of renal function.13,14,21–24 However, there are few studies comparing the renoprotective profile of levosimendan with that of dobutamine in patients with AHF.13,14 The randomized controlled LIDO trial21 reported a significant reduction of 9% in creatinine level in patients with almost normal renal function when treated with levosimendan as opposed to dobutamine. In patients with moderate renal impairment, levosimendan was found to have a more robust effect on eGFR, with an increase of 45% at 72 hours, compared with dobutamine infusion.21 Similarly, the nonrandomized PORTLAND study22 assessed the efficacy and safety of levosimendan in the treatment of AHF in everyday clinical practice. There was rapid improvement in diuresis in previously oliguric patients after beginning levosimendan, along with a reduction in serum creatinine levels that persisted at five days.22 Yilmaz et al.13 investigated 88 consecutive patients with AHF (NYHA class III-IV) who required inotropic therapy. Patients were randomized to receive either levosimendan or dobutamine. While LVEF increased significantly in both treatment groups, the levosimendan group showed significant improvement in eGFR after 24 hours (+15.3%), while the dobutamine arm showed no difference (-1.33%).13 The same group also compared the effects of levosimendan and dobutamine on right ventricular function in 40 consecutive patients with severe chronic biventricular dysfunction and showed that right ventricular function improved more in patients receiving levosimendan.14 Furthermore, in these patients levosimendan improved both 24-hour urine output and creatinine levels, whereas dobutamine produced only a small increase in urine output and no decrease in creatinine levels.14 The beneficial effect of levosimendan on renal function extends beyond AHF, according to two recent meta-analyses, in acute critically ill patients and in the perioperative setting, that showed a reduction in kidney injury.25,26
In agreement with these findings, our study, which aims to describe a real-world AHF population, showed that, even though eGFR was similar in the two groups at admission, patients treated with levosimendan had a lower incidence of CRS (49% vs. 77%). Furthermore, renal function recovery at discharge was incomplete in individuals who received dobutamine, unlike in patients selected for levosimendan perfusion, who had a complete recovery.
The mechanisms underlying levosimendan's renoprotective effect in patients with AHF are not fully understood. Improved hemodynamics, and hence increased kidney perfusion, could play an important role.24 However, in multivariate analysis, levosimendan therapy was shown to predict improved renal function independently of changes in left ventricular performance, suggesting that other factors may be responsible.23 Different possible renoprotective mechanisms of levosimendan have been proposed: an increase in renal blood flow due to hemodynamic improvement,27,28 additional increases in renal perfusion via vasodilation through KATP channel agonism,29 reversal of AT-2-mediated mesangial cell contraction with a consequent increase in glomerular capillary surface area and glomerular filtration rate,24 and possible anti-inflammatory properties, suggesting that it may protect against tubular injury.30 However, systemic venodilation together with pulmonary vasodilation, improving right ventricular performance, is probably the main mechanism distinguishing the effect on renal function of this drug from that of dobutamine.13 Moreover, the formation of an active metabolite of levosimendan may account for the prolonged effect of this drug.31
Nevertheless, in our study some differences between the groups may preclude firm conclusions. Patients in the dobutamine group appeared to present in a more severe condition, as expressed by lower systolic blood pressure, lower hemoglobin levels and older age, and generally requiring more multi-organ support. On the other hand, lower systolic blood pressure may itself have influenced the choice of the inotrope by the admitting physician, since the hypotensive effect of levosimendan lasts longer.21
In recent years, cystatin C has received considerable attention as a potential alternative to serum creatinine for estimating kidney function, and has consistently proved a better risk marker than creatinine, especially in acute scenarios.32 In our study, admission cystatin C, but not creatinine or BUN, was an independent predictor of CRS during hospital stay. Identifying individuals at risk for developing CRS by assessing cystatin C could help the physician provide a more tailored therapeutic strategy, with a view to decreasing CRS incidence and hence improving this population's dire prognosis.
Although multivariate analysis showed the use of dobutamine was associated with a five-fold higher risk of in-hospital mortality, these results need to be assessed with caution, since they conflict with those obtained in large clinical trials comparing the impact of levosimendan and dobutamine on mortality.33,34 However, these differences may be explained by the differences in systolic blood pressure at admission, since median systolic blood pressure in the levosimendan group was over 100 mmHg. The inclusion of patients with low blood pressure in SURVIVE34 and REVIVE-II33 may have partly explained their results, since the beneficial effects of levosimendan in reducing central venous pressure and improving pulmonary congestion may be offset by a drop in blood pressure, which jeopardizes vital organ perfusion.35 Furthermore, a recent analysis of 25 meta-analyses in different clinical settings consistently showed benefits for levosimendan, with lower relative risk for mortality, which supports our results.36
Study limitationsOur study has several limitations. First, this was a single-center study with a relatively small sample size. A larger sample of patients from multiple centers would make the analysis more robust and objective. Second, the observational nature of the study means that the inotrope used and its doses were at the discretion of the attending physician. Furthermore, the lack of randomization created two heterogeneous populations that clearly differed in severity on admission, which precludes firm conclusions regarding the superiority of levosimendan or dobutamine in terms of renoprotective profile. Finally, although the MDRD formula is currently the preferred method for estimating renal function,17 it should be applied when renal function is stable, which is probably not the case for many patients admitted with AHF.
ConclusionsAlthough the differences between groups preclude firm conclusions, levosimendan appears to have some renoprotective effect, as it was associated with a lower incidence of CRS and better recovery of renal function at discharge. This outcome, together with recent publications showing the benefit of levosimendan in renal protection, support the potential role of this drug in the prevention and treatment of CRS. Furthermore, identification of patients at increased risk of renal dysfunction by assessing cystatin C may enable selection of patients for levosimendan treatment, minimizing the incidence of CRS and its indisputably negative impact on AHF prognosis.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interestThe authors have no conflicts of interest to declare.
