



Persistence of the left superior vena cava is rare, being found in 0.3–2% of the general population, and shows considerable anatomical variability. We report the case of a 64-year-old man with idiopathic dilated cardiomyopathy, admitted electively for implantation of a cardiac resynchronization therapy defibrillator. Access was achieved via the left cephalic vein, but the lead was seen to advance to the left of the spinal column. Contrast injection revealed a persistent left superior vena cava draining into the right atrium close to the coronary sinus ostium.
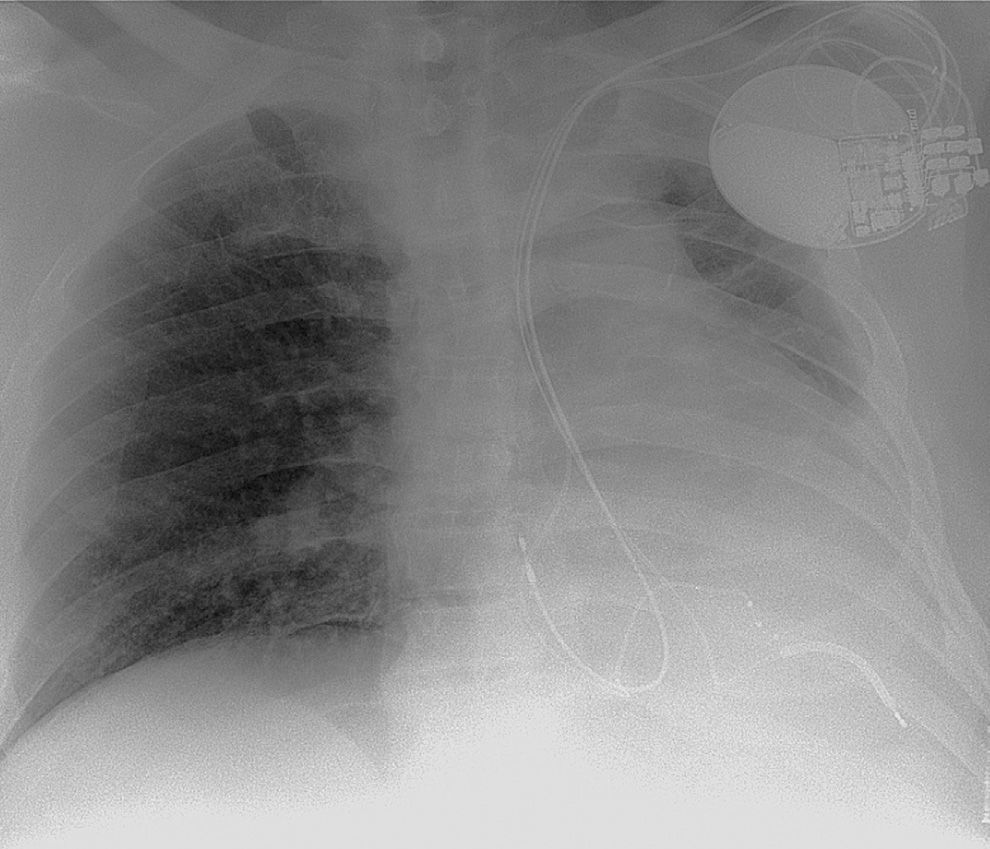
On encountering this congenital defect, many operators immediately decide to use special techniques, particularly for biventricular devices; some adopt a right approach to facilitate catheter manipulation, others use a hybrid technique (right and left in the same procedure), and some implant the right ventricular lead in the left ventricle. However, these techniques can be rather complex and carry an increased risk of infection and vascular injury, especially with a bilateral approach. Therefore, since according to various authors and our own experience conventional implantation can be safe and effective, it was decided to attempt this approach first. All the leads were positioned by the conventional technique, including a quadripolar lead in the coronary sinus (Figure 1).
At three-month follow-up stimulation thresholds were satisfactory and effective resynchronization had been achieved. In conclusion, although persistence of the left superior vena cava hampers implantation, the simplest approach should be attempted first.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of dataThe authors declare that no patient data appears in this article.
Right to privacy and informed consentThe authors declare that no patient data appears in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Nobre Menezes M, Bernardes A, de Sousa J, et al. Implantação de CRT-D através de veia cava superior esquerda persistente. Rev Port Cardiol. 2015;34:297–298.
