
Recurrent syncope has a significant impact on quality of life. The development of measurement scales to assess this impact that are easy to use in clinical settings is crucial. The objective of the present study is a preliminary validation of the Impact of Syncope on Quality of Life questionnaire for the Portuguese population.
MethodsThe instrument underwent a process of translation, validation, analysis of cultural appropriateness and cognitive debriefing. A population of 39 patients with a history of recurrent syncope (>1 year) who underwent tilt testing, aged 52.1±16.4 years (21–83), 43.5% male, most in active employment (n=18) or retired (n=13), constituted a convenience sample. The resulting Portuguese version is similar to the original, with 12 items in a single aggregate score, and underwent statistical validation, with assessment of reliability, validity and stability over time.
ResultsWith regard to reliability, the internal consistency of the scale is 0.9. Assessment of convergent and discriminant validity showed statistically significant results (p<0.01). Regarding stability over time, a test-retest of this instrument at six months after tilt testing with 22 patients of the sample who had not undergone any clinical intervention found no statistically significant changes in quality of life.
ConclusionsThe results indicate that this instrument is of value for assessing quality of life in patients with recurrent syncope in Portugal.
A síncope recorrente tem um impacto significativo na qualidade de vida. O desenvolvimento de escalas de medida de fácil aplicabilidade clínica para avaliar este impacto é fundamental. O objetivo do presente estudo é a validação preliminar do questionário Impact of Syncope on Quality of Life, para a população portuguesa.
MétodosO instrumento foi submetido a um processo de tradução, validaçãol, adequação cultural, e cognitive debriefing. Participaram 39 doentes com história de síncopes recorrentes (> 1ano de evolução), submetidos a teste de inclinação em mesa basculante (teste de tilt), que constituíram uma amostra de conveniência, com idade de 52,1±16,4 anos (21-83; 43,5% do sexo masculino), a maioria com uma situação profissional ativa (n=18) ou reformados (n=13). A versão portuguesa resultou numa versão semelhante unidimensional à original com 12 itens agregados num único somatório, tendo passado por validação estatística, com avaliação da fidelidade, validade e estabilidade no tempo.
ResultadosEm relação à fidelidade, a consistência interna da escala é de 0,9. Avaliámos a validade convergente, tendo obtido resultados estatisticamente significativos (p<0,01). Avaliámos a validade divergente tendo obtido resultados estatisticamente significativos. Relativamente à estabilidade no tempo foi efetuado um teste-reteste do instrumento aos seis meses após o teste de inclinação com 22 doentes desta amostra não submetidos a intervenção clínica, que não mostrou alterações estatisticamente significativas da qualidade de vida.
ConclusõesOs resultados obtidos indicam a pertinência da utilização deste instrumento em contexto português na avaliação da qualidade de vida de doentes com síncope recorrente.
According to the European Society of Cardiology guidelines, syncope is defined as a transient loss of consciousness due to global cerebral hypoperfusion characterized by rapid onset, short duration, and spontaneous complete recovery.1 According to the same source, in some forms there may be prodromes, including lightheadedness, nausea, sweating, weakness, and visual disturbances. Diagnosis is based on an initial assessment and diagnostic tests, including tilt testing. The prevalence of syncope in the general population is high, the first episode generally occurring between the ages of 10 and 30, and with greater frequency in females.2,3 The causes are diverse, the most common types being reflex (neurally mediated) syncope, syncope secondary to orthostatic hypotension and cardiac syncope.4 With regard to prognosis, it is necessary to consider risk of death, life-threatening events, recurrence of syncope and physical injury.
Recurrent syncope has a considerable impact on quality of life, similar to that of chronic diseases such as severe rheumatoid arthritis, chronic low back pain and mental illness.5,6 The development of measurement scales to assess this impact, as well as the effect of treatment, that are easy to use in clinical settings is therefore crucial. Such assessments include generic measures that can be applied to a range of diseases and cover various quality of life domains, and specific measures assessing syncope-related clinical domains and identifying changes in symptoms. The instrument most often used to assess quality of life in syncope is a general tool, the Medical Outcomes Study 36-item Short-Form Health Survey (SF-36), but this does not assess the clinical domains associated with syncope. Another general instrument often used is the EuroQol EQ-5D, which like all general tools does not measure the effects of lifestyle restrictions and apprehension on patients’ activities, such as driving.7 There is thus a need for instruments that specifically assess the impact of syncope on daily activities. One candidate is the Syncope Functional Status Questionnaire (SFSQ).8 However, according to Van Dijk et al.,9 although this instrument has high internal consistency, its validity is only moderate and it has a large floor effect; they point out that these limitations may be due to the fact that the choice of items was based on clinicians’ judgment. Since there are few other specific instruments assessing syncope, in 2009 the Impact of Syncope on Quality of Life (ISQL) was developed, an impact scale based on patient-centric analysis.7 As this has not been translated into Portuguese, we chose it for validation in the Portuguese population. With the current trend towards internationalization of clinical trials and comparison of results of clinical interventions between countries, there is an increasing need for measurement scales to be translated.10 However, since the domains assessed by these instruments are culturally specific, their application in different cultures will affect the results and how these are interpreted unless they have undergone transcultural validation. The objective of the present study is a preliminary validation of the ISQL questionnaire for the Portuguese population.
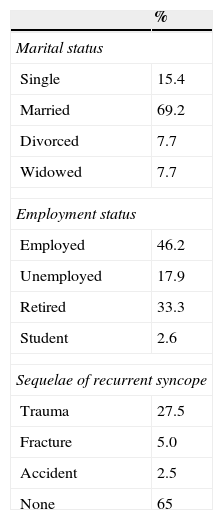
MethodsPopulationThe population consisted of 39 consecutive patients with a history of recurrent syncope (>1 year) who underwent tilt testing. Exclusion criteria were dementia, inability to communicate, and refusal to participate. Mean age was 52.1±16.4 years (21–83); 56.4% were female and 43.5% male, 69.2% were married, and most were in active employment (n=18) or retired (n=13) (Table 1).
A subgroup of 22 of these patients, with similar characteristics to the overall sample and who had not received any specific treatment for syncope and continued to suffer recurrent syncope, were assessed at six months after tilt testing. The mean age of this group was 52.8±16.2 years (29–78); 63.6% were female and 36.4% male.
Measurement scaleIn 2009, Rose et al. developed a new syncope-specific measure of health-related quality of life, the ISQL.7 The original version consists of 12 items rated on Likert scales11 in a single domain, based on patients’ perception of their clinical state over the previous four weeks, and measuring the impact of syncope on the patient's life, fear, depression, and physical limitations in a single score. The ISQL is a brief specific measure that is ideal for use in clinical practice.
Validation procedureThe present study tested the transcultural validity of the ISQL in a Portuguese sample. The instrument underwent a process of translation, translation revision, discussion of content validity and construct validity, analysis of the complexity of the questions and of cultural appropriateness, cognitive debriefing, and general revision of the scale. In the first step, translation and back-translation by two bilingual health professionals working independently produced a Portuguese version of the questionnaire, the clarity of which was then evaluated by the authors, and it was then passed to an expert panel, composed of two cardiologists and two clinical psychologists, who reviewed its appropriateness for patients with syncope. The results were analyzed in terms of the number of agreements and disagreements among the expert panel and the translated version was reformulated accordingly. The resulting pilot version was applied to a group of 10 individuals of both sexes and different ages with similar characteristics to the target population in order to confirm that the questionnaire was easy to understand. No item appeared to need further editing as the instrument was generally considered by the participants to be useful and accessible, and the final Portuguese version of the ISQL (Annex 1) can thus be considered clear and comprehensible. Like the original, it has 12 items giving a single aggregate score, and has undergone statistical validation, with assessment of reliability, validity and stability over time. Patients with a history of recurrent syncope (>1 year) who had undergone tilt testing at Hospital Santa Marta were contacted and a total of 39 agreed to participate and completed the questionnaire. Of these, 22 who had not undergone any clinical intervention to treat syncope in the meantime repeated the questionnaire six months after tilt testing.
Statistical analysisThe collected data were treated as a single sample. Descriptive statistics were used to analyze the population and nominal measures (gender, marital status, employment status and sequelae of recurrent syncope), expressed as frequencies. Continuous measures (age, number of syncopal episodes) were analyzed by descriptive statistics using measures of central tendency (mean), dispersion (standard deviation), maximum and minimum. Psychometric properties were assessed by Cronbach's alpha to measure the reliability of the questionnaire. Validity was tested by Pearson's correlation for convergent validity (correlation between the ISQL and health perception as assessed by the SF-36 and the visual and numerical scale of the Multiple Sclerosis Quality of Life [MSQOL-54]) and ANOVA for divergent validity (comparison of the ISQL with age and marital status). Stability over time was assessed by a test-retest at six months. The statistical analysis was carried out using SPSS version 17.
ResultsAnalysis of the instrument's psychometric properties covered reliability, validity and stability over time.
With regard to reliability, the internal consistency of the scale is 0.9.
Convergent validity was analyzed by relating the ISQL to items assessing health perception in the SF-36 and the MSQOL-54, using these as measures of quality of life. Statistically significant correlations were obtained with the health perception item in the SF-36 (r=0.45; p<0.01) and with the MSQOL-54 (r=0.44; p<0.01).
Divergent validity was assessed by comparing the ISQL with age and marital status; no statistically significant results were obtained.
For stability over time, a test-retest of the ISQL at six months after tilt testing with 22 patients of the sample who had not undergone any clinical intervention found a statistically significant correlation (r=0.46; p<0.05).
DiscussionThe results of this validation study of the ISQL suggest that the Portuguese version, like the original, is a valid and reliable instrument to assess quality of life and degree of restrictions on patients’ activities resulting from recurrent syncope. It was also shown to be easy to apply.
The high value obtained for internal consistency clearly demonstrates its reliability. This property was not assessed in the original study, which the authors admitted was a limitation.7
Convergent validity, measured by the correlation of the ISQL with two items from other scales evaluating quality of life, showed statistically significant results, validating this instrument for assessment of quality of life, as in the original study.7
Divergent validity, measured by comparing the ISQL with two variables from the sample characteristics (age and marital status), was not statistically significant, as in the original study,7 demonstrating that the instrument focuses on other variables, such as those used in the analysis of convergent validity, i.e. those that measure the impact of recurrent syncope on quality of life.
The scale was shown to be stable over time, presenting a moderate correlation in quality of life assessment over a period of six months after tilt testing in stable patients who had not undergone clinical intervention during that period. This parameter was also not analyzed in the original study, another limitation pointed out by the authors.7
Like the authors of the original study, we stress the need to evaluate the sensitivity of the ISQL to change in clinical state in a group who underwent clinical intervention during follow-up.7 It would be useful for such an instrument to measure patients’ perceptions of their health status, providing a direct quantification of the perceived clinical benefits of treatments they have undergone and reducing inter-observer variability.
Other limitations of the present study include the small sample, for reasons beyond the authors’ control, and the fact that only 22 patients agreed to complete the questionnaire again after six months. Also, the number of syncopal episodes in the four weeks prior to application of the questionnaire (the time frame of the instrument) was not quantified, either at the time of tilt testing or six months later in patients who had not undergone clinical intervention and had remained symptomatic.
It would be useful for this instrument to be translated into other languages, in order to perform multicultural studies, and to apply it to a larger number of patients, to strengthen the statistical power of its psychometric properties.
ConclusionsAnalyzing the results of the present study, we conclude that the ISQL is of value for assessing quality of life in patients with recurrent syncope in Portugal.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interestThe authors have no conflicts of interest to declare.
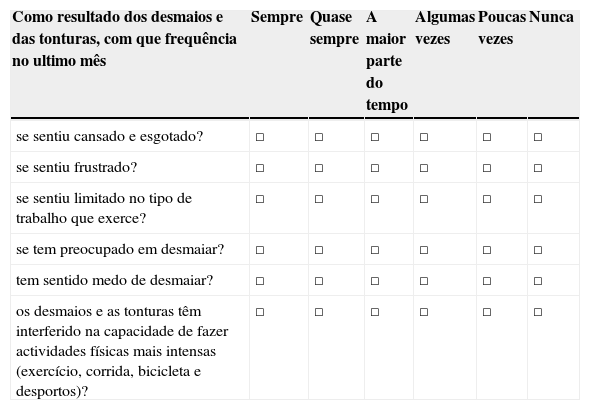
As seguintes perguntas referem-se às dificuldades que tem sentido em consequência dos desmaios e tonturas. Por favor responda a cada pergunta assinalando com um X uma das caixas. Se estiver com dúvidas sobre como responder, é favor procurar a melhor resposta possível.
| Como resultado dos desmaios e das tonturas, com que frequência no ultimo mês | Sempre | Quase sempre | A maior parte do tempo | Algumas vezes | Poucas vezes | Nunca |
|---|---|---|---|---|---|---|
| se sentiu cansado e esgotado? | □ | □ | □ | □ | □ | □ |
| se sentiu frustrado? | □ | □ | □ | □ | □ | □ |
| se sentiu limitado no tipo de trabalho que exerce? | □ | □ | □ | □ | □ | □ |
| se tem preocupado em desmaiar? | □ | □ | □ | □ | □ | □ |
| tem sentido medo de desmaiar? | □ | □ | □ | □ | □ | □ |
| os desmaios e as tonturas têm interferido na capacidade de fazer actividades físicas mais intensas (exercício, corrida, bicicleta e desportos)? | □ | □ | □ | □ | □ | □ |
| Pense no ultimo mês e indique o quanto concorda com as seguintes afirmações: | Concordo | Concordo mais ou menos | Nem concordo nem discordo | Discordo mais ou menos | Discordo |
|---|---|---|---|---|---|
| Em consequência dos desmaios, realizo menos do que queria. | □ | □ | □ | □ | □ |
| Ninguém percebe o efeito que os desmaios têm na minha vida. | □ | □ | □ | □ | □ |
| Os desmaios deixam-me confuso. | □ | □ | □ | □ | □ |
| Pense no último mês e indique com que frequência tem evitado | Sempre | Quase sempre | A maior parte do tempo | Às vezes | Poucas vezes | Nunca |
|---|---|---|---|---|---|---|
| conduzir um veículo | □ | □ | □ | □ | □ | □ |
| ficar em pé durante longos períodos de tempo (por exemplo mais que 5 minutos) com receio de desmaiar. | □ | □ | □ | □ | □ | □ |
| estar em ambientes quentes ou abafados com receio de desmaiar. | □ | □ | □ | □ | □ | □ |
Please cite this article as: Nave-Leal E, Oliveira M, Pais-Ribeiro J, et al. Impacto da síncope na qualidade de vida: validação duma escala de avaliação em doentes submetidos a teste de inclinação em mesa basculante. Rev Port Cardiol. 2015;34:173–177.
