







Vascular inflammation plays a crucial role in the pathogenesis of atherosclerosis and mediates various stages of atherosclerotic plaque development, from lipid streak formation to the plaque rupture and destabilization that precedes the clinical syndromes of cardiovascular disease. Inflammatory biomarkers constitute valuable tools to study this process, enabling the effects of different therapeutic interventions to be assessed. Currently, C-reactive protein (CRP) determined by high-sensitivity methods (hs-CRP) is the most extensively studied biomarker. Data regarding hs-CRP and cardiovascular risk, though largely consistent, are of unclear clinical relevance. This article provides a comprehensive review of current knowledge concerning cardiovascular risk and hs-CRP, and concludes with an evidence-based analysis of the current role of hs-CRP in cardiovascular risk assessment.
A inflamação vascular tem um papel crucial na patogénese da aterosclerose e medeia vários dos estadios de desenvolvimento da placa de ateroma, desde a formação da estria lipídica à destabilização e rotura da placa que precede as síndromes clínicas da doença cardiovascular. Os biomarcadores inflamatórios constituem uma ferramenta valiosa para acompanhar a evolução deste processo, permitindo mensurar o efeito das diversas atitudes terapêuticas implementadas. Neste contexto, a proteína C reativa (PCR), determinada por métodos de alta sensibilidade (PCR-as), é o biomarcador mais extensamente estudado. Os dados relativos à associação entre PCR-as e risco cardiovascular são amplamente consistentes, embora apresentem relevância clínica incerta. Este artigo fornece uma revisão abrangente da evidência existente sobre PCR-as e risco cardiovascular, no que respeita a prevenção primária e secundária, e conclui com uma análise baseada na evidência sobre o papel atual da PCR-as na avaliação do risco cardiovascular.
Atherosclerosis, once considered to result from a passive process of lipid accumulation, is now known to be an active process of cell activation, inflammation and thrombosis.1 Inflammation is the key mechanism in the pathogenesis of the different stages of atherosclerosis, from onset, progression of atheroma, plaque instability and rupture, and restenosis following angioplasty.2–4 The inflammatory process is exacerbated by the cardiovascular risk factors identified in epidemiological studies, particularly elevated LDL cholesterol.1 There is mounting evidence that modifying these risk factors reduces inflammation and thus helps prevent atherosclerotic events.5
However, the inflammatory process of atherosclerosis is difficult to measure directly. No imaging techniques can assess inflammatory changes, and arterial biopsy to monitor such alterations or therapeutic interventions is neither practical nor ethical. There is therefore a growing interest in biomarkers of inflammation, plasma proteins that can by quantified in peripheral blood.
The explosion in inflammatory biomarkersInflammatory biomarkers provide useful information on the inflammatory process of atherosclerosis; they act as a window into the process of cell activation, recruitment of inflammatory cells and proliferation.6 They may be produced by inflammatory and vascular cells in the plaque or, indirectly, in organs such as the liver and spleen. However, as it is a non-specific process, inflammation in other tissues or organs raises levels of inflammatory biomarkers, which can confound the relationship between plasma levels of these biomarkers and the inflammation associated with stable atherosclerotic syndromes. There was thus a need for high-sensitivity methods to detect small variations in plasma concentrations of these molecules in uninfected individuals that could be related to the inflammatory process of atherosclerosis. Assessment of inflammatory biomarkers complements the study of markers of tissue damage (troponin), of thrombosis and thrombolysis (tissue plasminogen activator) and of lipid oxidation (oxidized LDL). Together, these biomarkers provide crucial information on the atherosclerotic process. Of the large and ever-growing list of inflammatory biomarkers (Table 1), C-reactive protein (CRP) is the most thoroughly studied in coronary artery disease (CAD), and is the subject of this review.
Inflammatory markers.
| Cytokines | |
| Primary inflammatory cytokines | IL-1; TNF-α |
| Secondary inflammatory cytokines | IL-6 |
| Chemokines | IL-8; MCP-1 |
| Adhesion molecules | |
| Selectins | P-, E-, L-selectin |
| Cell adhesion molecules | ICAM-1; VCAM-1 |
| Acute phase proteins | |
| Produced in high concentrations | CRP; serum amyloid A |
| Produced in low concentrations | Fibrinogen |
In recent decades, over 30 epidemiological studies have shown that CPR is associated with cardiovascular risk.7 The molecule has characteristics that make it a particularly attractive subject of study: as a positive acute phase protein it is a marker of systemic inflammation that increases in response to various types of injury, particularly bacterial infections, that function as inflammatory stimuli.8 Its production in the liver is induced mainly by interleukin-6 (IL-6) and, unlike other acute phase markers, its levels are relatively stable, with no significant diurnal variation, and can thus be accurately measured.9 During the 1990s high-sensitivity techniques were developed to detect lower serum CRP levels than by previous laboratory methods (down to 0.3mg/l), known as high-sensitivity CRP (hs-CRP), and these techniques should be used when assessing the cardiovascular risk associated with the chronic vascular inflammation of atherosclerosis.There is growing evidence that CRP is not merely a marker of inflammation, but also plays an active role in atherogenesis (Figure 1).10,11 In 2003, Ishikawa et al. concluded that CRP is found inside atherosclerotic plaques and plays an important part in both plaque instability and post-angioplasty restenosis.10 Similarly, Inoue et al. demonstrated in 2005 that CRP is released by atherosclerotic plaques responsible for acute coronary syndromes (ACS).11 They also showed that there is a CRP gradient in the coronary circulation proximal and distal to the plaque and a transcardiac gradient (from coronary sinus to peripheral blood) that gradually increases after angioplasty, peaking at 48hours, suggesting a cardiac origin of CRP.11 CRP levels correlate directly with various cardiovascular risk factors, including body mass index, smoking, systolic blood pressure (BP), levels of triglycerides and total cholesterol, heart rate, fasting blood glucose and history of CAD or stroke, and inversely with HDL cholesterol and diastolic BP, in both children and adults.12–14
CRP and primary prevention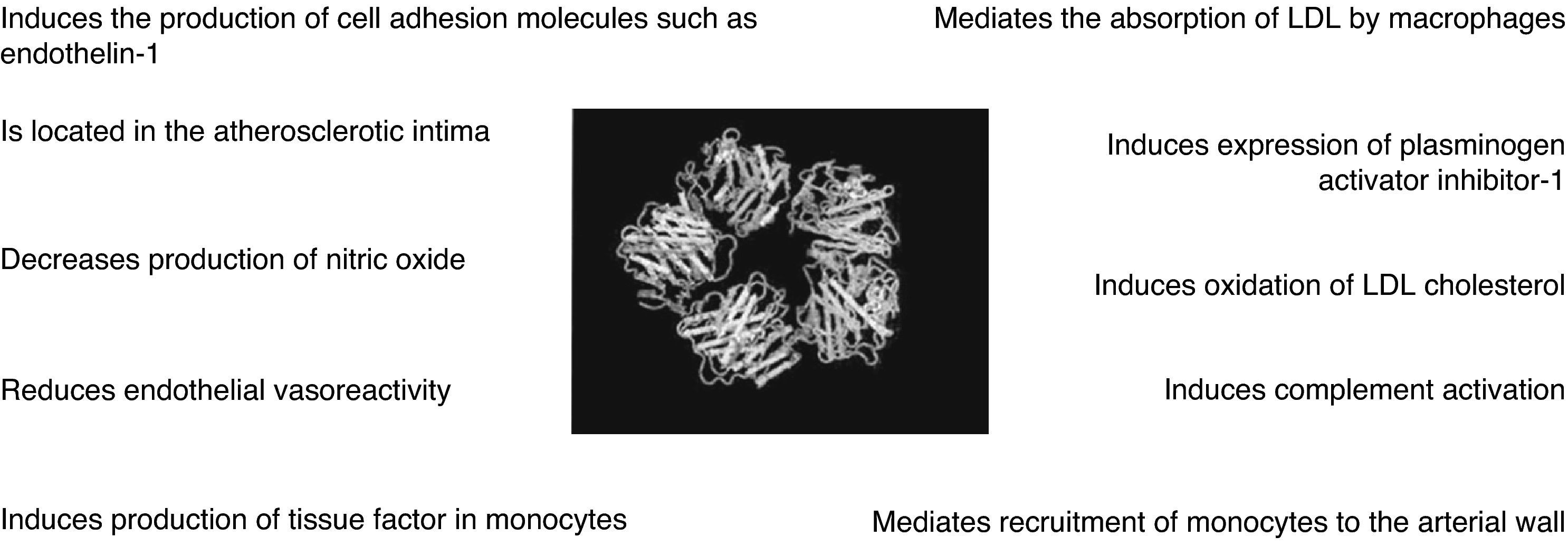
Several prospective trials in apparently healthy individuals have shown that elevated hs-CRP is positively correlated with cardiovascular morbidity and mortality. The MRFIT study (Multiple Risk Factor Interventional Trial) concluded that increased hs-CRP predicted higher risk for cardiovascular disease in middle-aged men, although the association was only statistically significant for smokers.15 The Physician's Health Study (PHS), a controlled prospective study of individuals without cardiovascular disease and including a low percentage of smokers, showed that those with higher baseline hs-CRP had double the risk of stroke, three times higher risk of myocardial infarction (MI), and four times higher risk of severe peripheral arterial disease. Cardiovascular risk was not affected by smoking or lipid levels.16 The MONICA Augsburg prospective study of 936 healthy middle-aged individuals with no clinical evidence of CAD showed a 19% greater risk of fatal and non-fatal coronary events for each increment of standard deviation after adjustment for various cardiovascular risk factors, including smoking.17 In the prospective PREVEND study of 8139 individuals without previous documented CAD, followed for the incidence of coronary angiography and coronary events from 1997 to 2003, hs-CRP levels were associated with angiographic characteristics and clinical consequences of plaque instability during follow-up.18 The Women's Health Study (WHS), of post-menopausal women, concluded that hs-CRP was the best predictor of cardiovascular risk compared to other factors including lipid levels and homocysteine. A subgroup analysis of women with LDL cholesterol <130mg/l, traditionally considered to be low risk, showed that those with higher hs-CRP were at greater risk for future acute events. Follow-up of the total population revealed that hs-CRP was a strong predictor of cardiovascular events and better than LDL cholesterol.19,20 On the basis of the PHS and WHS studies, adjusted relative risk of cardiovascular events increases by 26% in men and 33% in women for each quartile of hs-CRP.21
Ridker et al. assessed the ability of non-traditional risk factors to predict cardiovascular events in a population of 24558 healthy women, and on this basis developed a cardiovascular risk score, the Reynolds risk score, which reclassified 40–50% of women previously classified as intermediate risk as high or low risk. The simplified score includes age, systolic BP, hemoglobin A1c, smoking, total and HDL cholesterol, hs-CRP and family history of premature MI (at under 60 years of age), and has greater prognostic accuracy than conventional risk scores.22 A similar score, also including hs-CRP and family history of MI, was assessed in men, and also has significantly better ability than traditional models to predict overall cardiovascular risk.
A 2003 study assessed the relation between hs-CRP, the presence of metabolic syndrome and cardiovascular events (MI, stroke, coronary revascularization and cardiovascular death) in 14719 apparently healthy women, 24% with metabolic syndrome, in an 8-year follow-up. Briefly, hs-CRP levels predicted cardiovascular events, particularly in those with metabolic syndrome at inclusion in the study24; this conclusion was confirmed in a subsequent study.25 As well as thrombotic events, hs-CRP levels also predicted type 2 diabetes,26 a disease that shares certain inflammatory mechanisms with atherosclerosis. This may have implications for the choice of therapeutic targets in diabetes control. Finally, hs-CRP appears to be of value in screening children at risk for developing CAD as adults.27
These data suggest that hs-CRP levels add prognostic value to classic risk factors including lipid parameters, and help identify patients at risk for cardiovascular events, even those previously classified as low or intermediate risk.
However, there is not complete consensus regarding these findings. Other studies have concluded that the predictive power of hs-CRP alone and in association with conventional risk factors is relatively low.28–31 According to these authors, the focus in clinical practice should continue to be on classic risk factors such as BP, lipids, and smoking. In a 2010 study of the contribution of 30 biomarkers to cardiovascular risk estimation, Blankenberg et al. concluded that none of the biomarkers under study, including hs-CRP, provided additional prognostic value compared to traditional risk scores. However, adding a score based on three biomarkers (hs-CRP, troponin I and BNP) to a conventional risk model improved estimation of 10-year risk for cardiovascular events in two middle-aged European populations (Table 2).32
Main studies of primary prevention.
| Study | Design | Population | Main results |
| Kuller et al., 199615 (MRFIT) | Prospective | 491 AH men | hs-CRP predicted cardiovascular death (statistically significant only for smokers). |
| Ridker et al., 199716 (PHS) | Prospective | 543 AH men | hs-CRP predicted stroke, MI and severe peripheral arterial disease. |
| Koenig et al., 199917 (MONICA Augsburg) | Prospective | 936 AH men | 19% increase in risk for fatal and non-fatal coronary events for each increment in standard deviation of hs-CRP. |
| Geluk et al., 200818 (PREVEND) | Prospective | 8139 AH men and women | hs-CRP levels were associated with angiographic characteristics and clinical consequences of plaque instability. |
| Ridker et al., 200019 (WHS) | Prospective | 28263 AH post-menopausal women | hs-CRP was the strongest predictor of cardiovascular risk even in women with LDL cholesterol <130 mg/l. |
| Ridker et al., 200220 | Prospective | 27939 AH women | hs-CRP was a better predictor of cardiovascular risk than LDL cholesterol and added prognostic information to the Framingham score. |
| Ridker et al., 200722 | Prospective | 24558 AH women | The new Reynolds Risk Score, which includes hs-CRP, reclassifies 40-50% of women previously classified as intermediate risk as high or low risk and is superior to conventional risk scores. |
| Ridker et al., 200823 | Prospective | 10724 AH men | The Reynolds Risk Score for men, which includes hs-CRP, has significantly better ability to predict overall cardiovascular risk than traditional models. |
| Ridker et al., 200324 | Prospective | 14719 AH women (24% with metabolic syndrome) | hs-CRP identifies patients with metabolic syndrome at greater risk for cardiovascular events. |
| Danesh et al., 200429 | Prospective | 3969 AH men and women | hs-CRP has only moderate ability to predict cardiovascular events and is not significantly superior to classic risk factors. |
| Lloyd-Jones et al., 200630 | Meta-analysis of prospective studies (1966–2005) | Ability of hs-CRP to predict cardiovascular events is not superior to the Framingham score. In those with moderate cardiovascular risk (10–20% risk at 10 years) hs-CRP >3.0mg/l can indicate greater risk | |
| Wang et al., 200631 | Prospective | 3209 AH men and women | hs-CRP has only moderate ability to predict cardiovascular events additional to classic risk factors. |
| Blankenberg et al., 201032 | Prospective | 7915 AH men and women | hs-CRP has no more prognostic value than traditional risk scores. |
| Ridker et al., 200164 (AFCAPS/TexCAPS) | Randomized prospective | 5742 AH men and women | Individuals with elevated hs-CRP, independently of cholesterol levels, had greater cardiovascular risk and benefited from allocation to the lovastatin group. |
| Albert et al., 200165 (PRINCE) | Randomized prospective | 1702 AH men and women | Pravastatin reduced hs-CRP levels in individuals with no prior history of cardiovascular disease, irrespective of cholesterol levels. |
| Ridker et al., 200870 (JUPITER) | Randomized prospective | 17802 AH men and women (with LDL cholesterol <130mg/dl and hs-CRP >2mg/l) | Rosuvastatin reduced the primary endpoint of MI, hospitalization for UA, revascularization, stroke and cardiovascular death compared to placebo. |
| Mora et al., 201071 (JUPITER substudy) | Randomized prospective | 17802 AH men and women (with LDL cholesterol <130mg/dl and hs-CRP >2mg/l) | There was no significant difference in treatment effect between the sexes (42% in men and 46% in women). |
AH: apparently healthy; CAD: coronary artery disease; hs-CRP: high-sensitivity C-reactive protein; MI: myocardial infarction; UA: unstable angina.
To summarize, as measurement of hs-CRP in primary prevention is not consensual and it is not clear whether its superior predictive ability is clinically relevant by helping reduce cardiovascular morbidity and mortality, large-scale validation trials are required before it should be used in routine clinical practice.33
CRP and secondary preventionStable coronary artery diseaseIt has been consistently demonstrated that hs-CRP is a marker of adverse events in patients with stable CAD. However, there is disagreement concerning hs-CRP levels and severity of CAD as assessed by invasive or computed tomography angiography, with some studies supporting34–36 and others denying37–39 an association. It has been shown that hs-CRP levels correlate inversely with degree of coronary collateral circulation.40,41
A 2006 study by Sinning et al. assessing the impact of hs-CRP and fibrinogen on cardiovascular prognosis of patients with stable CAD concluded that inflammatory markers have some prognostic value but add little to that of traditional risk factors.42 A substudy of the placebo-controlled randomized Prevention of Events with Angiotensin-Converting Enzyme Inhibition (PEACE) trial of 3771 patients followed for a mean of 4.8 years, showed that hs-CRP >1mg/l was associated with significantly higher risk of cardiovascular death, MI and stroke, even after adjustment for patients’ baseline characteristics and current treatment.43
Other studies have shown that hs-CRP is inversely correlated with left ventricular ejection fraction and is an independent predictor of worsening New York Heart Association (NYHA) functional class in patients with CAD referred for elective coronary angiography, irrespective of CAD severity.44 These authors concluded that hs-CRP was an independent predictor of adverse cardiac events (ACS and cardiovascular death) in patients with stable CAD irrespective of the presence of significant atherosclerotic lesions.45 This may be explained by arterial wall remodeling, which is known to be associated with the development of CAD; positive correlations have been demonstrated between hs-CRP and degree of coronary remodeling,46 and between hs-CRP and plaque composition, particularly the proportion of central necrotic tissue,47 as assessed by intravascular ultrasound in patients with CAD referred for elective coronary angiography.
Inflammatory markers have also been shown to be predictors of recurrent events following MI. In a 1998 study of 391 patients, Ridker et al. concluded that high levels of inflammation measured by hs-CRP and serum amyloid A (SAA) predicted recurrence of adverse events; patients in the highest quartile of hs-CRP levels had 75% higher risk of recurrence than those in the lowest quartile (p=0.02 for both CRP and SAA). Interestingly, lipid levels were similar in those with and without evidence of inflammation.48 Furthermore, serum hs-CRP levels also independently predicted rapid progression of CAD. This association was also suggested in 2004 by Zouridakis et al. in a study of 124 patients with CAD awaiting elective coronary angiography (mean waiting time of 4.8 months): rapid progression of CAD (defined as ≥10% diameter reduction of a pre-existing stenosis ≥50%, ≥30% diameter reduction of a stenosis <50%, development of a new stenosis ≥30% in a previously normal segment, or progression of any stenosis to total occlusion) occurred in 35 patients (28%).49
Finally, hs-CRP levels correlate with myocardial ischemia induced by stress testing. Ischemia was more likely to be induced in patients in the highest hs-CRP quintile (>3.8mg/l) than those in the lowest (<0.7mg/l; 75% vs. 38%).50 It should be noted that this association was only significant in patients not taking statins or beta-blockers.
Unstable coronary artery diseaseIt is now known that hs-CRP levels correlate with the presence of unstable plaque documented by carotid Doppler study51 and with increased temperature in such plaques as measured by a thermography catheter.52 However, their relation with extent of MI as assessed by elevated cardiac enzymes or ejection fraction is the subject of debate.53,54
In the context of ACS, hs-CRP has consistently proved a marker of adverse cardiac events including MI, urgent revascularization, restenosis after percutaneous coronary intervention (PCI) and cardiovascular death. In the randomized Thrombolysis in Myocardial Infarction (TIMI 11A) trial, Morrow et al. showed that hs-CRP levels after ACS were significantly higher in patients who died during follow-up than in survivors (1.3mg/l vs. 0.72mg/l, p<0.001). They also independently predicted 14-day mortality, including in patients with negative troponin assay.55 In the Fragmin during Instability in Coronary Artery Disease (FRISC) trial, hs-CRP was an independent predictor of cardiovascular mortality, which was 5.7% in patients with hs-CRP of <2mg/l, 7.8% in those with hs-CRP between 2 and 10mg/l, and 16.5% in those with hs-CRP >10mg/l.56 In the Global Use of Strategies To open Occluded arteries IV (GUSTO-IV) trial, although a rise in hs-CRP was associated with increased 30-day mortality independently of troponin levels, it was not associated with recurrence of non-fatal ischemic events,57 and thus predicted mortality better than non-fatal ischemic events. In 2005, Foussas et al. concluded that hs-CRP levels had prognostic usefulness when added to the well-validated TIMI risk score for ST- and non-ST elevation MI and that both should be used to stratify risk in MI patients.58
hs-CRP has been found to be an independent predictor of mortality in patients with ACS even after early coronary revascularization. In a prospective study in 2002 of patients undergoing PCI following non-ST elevation MI, hs-CRP of >10mg/l at admission was associated with increased mortality in a 20-month follow-up.59 Another study, of 319 patients with ST-elevation MI treated by thrombolysis, revealed that those with elevated hs-CRP (third tertile) were more likely to have reperfusion failure and had higher in-hospital mortality.60 Similar results were obtained in 2008 by Hoffman et al., who studied the relationship between admission hs-CRP, myocardial reperfusion assessed by myocardial blush grade after crossing the culprit lesion, and prognosis in 191 patients undergoing PCI after non-ST elevation MI.61 Reperfusion was more often unsuccessful in patients with elevated hs-CRP (>5mg/l), and on multivariate analysis only hs-CRP levels and reperfusion failure were independent predictors of mortality during follow-up.61
However, in a prospective study of 1360 patients with stable and unstable (MI and unstable angina [UA]) CAD, the adjusted hazard ratio (HR) for MI/death for hs-CRP above the first tertile was 1.8 for stable angina, 2.7 for UA but only 1.0 for MI.62 A study by Bogaty et al. in ACS patients followed for one year concluded that baseline hs-CRP had only moderate predictive ability for the primary combined endpoint of death, non-fatal MI and UA, and even this disappeared after adjustment for common clinical variables (Table 3).63
Main studies of secondary prevention.
| Study | Design | Population | Main results |
| Sinning et al., 200642 (Athero Gene) | Prospective | 1806 patients with stable CAD | hs-CRP has prognostic value but adds little to that of traditional risk factors. |
| Sabatine et al., 200743 | Prospective | 3771 patients with stable CAD | hs-CRP values >1mg/l, even after adjustment for baseline characteristics and current treatment, were associated with significantly higher risk of cardiovascular death, MI and stroke. |
| Arroyo-Espliguero et al., 200945 | Prospective | 790 patients with CAD | hs-CRP was an independent predictor of adverse cardiac events (ACS and cardiovascular death) irrespective of the presence of significant atherosclerotic lesions. |
| Zouridakis et al., 200449 | Prospective | 124 patients with CAD | hs-CRP levels independently predicted rapid progression of CAD. |
| Morrow et al., 199855 (TIMI 11A substudy) | Prospective | 445 patients after ACS | hs-CRP levels were significantly higher in patients who died during follow-up. |
| Lindahl et al., 200056 (FRISC) | Prospective | 917 patients with ACS | hs-CRP was an independent predictor of cardiovascular mortality. |
| James et al., 200357 (GUSTO-IV) | Prospective | 7108 patients with ACS | A rise in hs-CRP during ACS was associated with increased 30-day mortality independently of troponin levels, but was not associated with recurrence of non-fatal ischemic events. |
| Foussas at al., 200558 | Prospective | 1846 patients with ACS | hs-CRP levels had prognostic usefulness added to the well-validated TIMI risk score for ST- and non-ST elevation MI. |
| Mueller et al., 200259 | Prospective | 1042 patients with non-ST elevation MI | hs-CRP >10mg/l at admission was associated with increased mortality in follow-up. |
| Zairis et al., 200260 | Prospective | 319 patients with ST elevation MI treated by thrombolysis | Elevated hs-CRP (third tertile) was associated with reperfusion failure and higher in-hospital mortality. |
| Nakachi et al., 200861 | Prospective | 191 patients with non-ST elevation MI treated by PCI | hs-CRP and reperfusion failure were independent predictors of mortality during follow-up. |
| Bogaty et al., 200863 (RISCA) | Prospective | 1210 patients with ACS | hs-CRP had only moderate predictive ability (primary combined endpoint of death, non-fatal MI and UA), and this disappeared after adjustment for common clinical variables. |
| Zebrack et al., 200262 | Prospective | 1360 patients with stable and unstable CAD | hs-CRP predicted the endpoint of MI/death in patients with stable and unstable angina but not in those with MI. |
| Ridker et al., 199848 (CARE) | Randomized prospective | 391 patients with fatal and non-fatal MI | In patients taking pravastatin, reduction of risk for coronary events was greater in those with evidence of inflammation as assessed by hs-CRP levels, irrespective of lipid levels. |
| Ridker et al., 200577 (PROVE-IT) | Randomized prospective | 3745 patients with ACS | Aggressive statin therapy reduces hs-CRP levels to less than 2mg/l, resulting in lower risk for MI and fatal coronary events, independently of reductions in LDL cholesterol. |
| Morrow et al., 200678 (Aggrastat-to-Zocor) | Randomized prospective | 3813 patients with ACS | hs-CRP levels 30 days and four months after MI are independently associated with long-term survival. More aggressive statin therapy is likely to result in low CRP. |
ACS: acute coronary syndromes; CAD: coronary artery disease; hs-CRP: high-sensitivity C-reactive protein; MI: myocardial infarction; UA: unstable angina.
On the basis of these data, it can be concluded that while hs-CRP has short- and long-term prognostic value in stable angina and UA and following MI, its usefulness is more debatable in the acute phase of MI, which suggests that it should be measured after the acute inflammatory reaction of MI, so as to ensure that the measurement reflects baseline values.
CRP and preventive therapy (primary and secondary)In vitro and in vivo studies have shown that CRP is not merely a marker of inflammation, but that it plays an active part in the development of the atherosclerotic plaque and subsequent plaque instability and thrombus formation. There has accordingly been extensive research into the relation between CRP and cardioprotective drugs. An analysis of the Air Force/Texas Coronary Atherosclerosis Prevention Study (AFCAPS/TexCAPS) showed that statin therapy as primary prevention directly lowers hs-CRP levels; individuals with high LDL cholesterol (irrespective of hs-CRP levels) and those with low LDL cholesterol but high hs-CRP were at greater risk of cardiovascular events during follow-up; the lovastatin group showed substantial benefit.64 In the PRINCE (PRavastatin Inflammation/CRP Evaluation) study, pravastatin reduced CRP levels in individuals with no prior history of cardiovascular disease.65
However, three meta-analyses of studies of statins in primary prevention concluded that they did not reduce total or coronary mortality in men or women,66–68 while in the Management of Elevated Cholesterol in the Primary Prevention Group of Adult Japanese (MEGA) study, in which many more women than men were enrolled, the reduction in events was significant only for men.69
The JUPITER (Justification for the Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin) study was a multicenter randomized double-blind trial in 17 802 apparently healthy individuals without hyperlipidemia (LDL cholesterol <130mg/dl) but hs-CRP >2mg/l, divided into two groups: rosuvastatin 20mg/day or placebo. Participants were followed for a mean of 1.9 years (maximum 5.0). Rosuvastatin reduced LDL cholesterol by 50% and CRP by 37%, and there were significantly fewer major cardiovascular events in the treatment group. The rate of the combined primary endpoint of stroke, MI, UA, coronary revascularization or cardiovascular death was 0.77 and 1.36 per 100 person/years of follow-up for the rosuvastatin and placebo groups, respectively (HR for the rosuvastatin group: 0.56; 95% confidence interval [CI]: 0.46–0.69; p<0.00001) (Figure 2).70 There was no significant difference in treatment effect between the sexes (42% in men and 46% in women).71
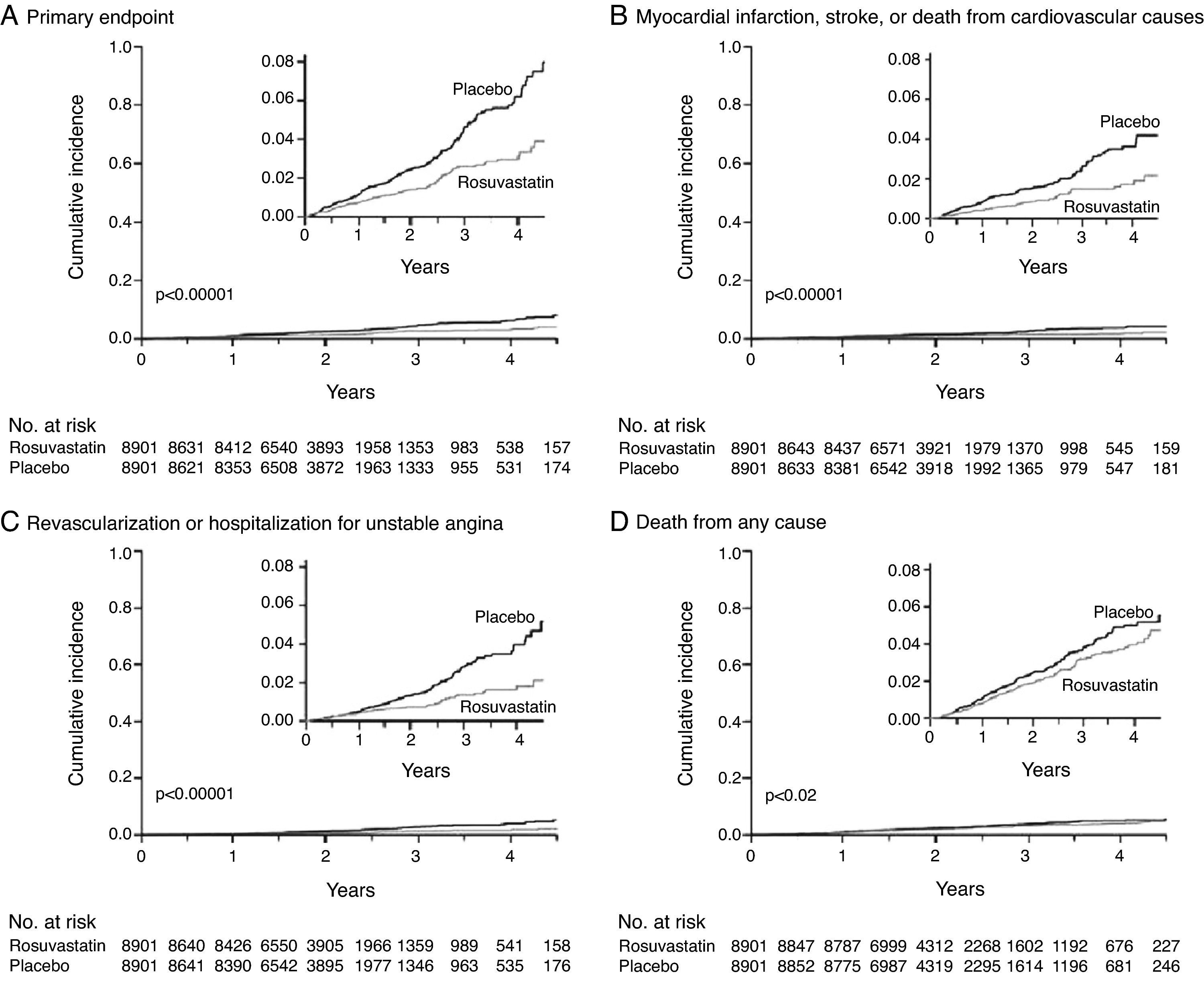
Rosuvastatin significantly reduced the incidence of major cardiovascular events in apparently healthy individuals without hyperlipidemia (LDL <130mg/dl) but with elevated high-sensitivity C-reactive protein (>2mg/l).
Two meta-analyses that included the JUPITER trial concluded that statin therapy reduced the relative risk of cardiovascular events and increased survival in both sexes.71,72
Some authors consider that preventive treatment with statins in patients with high hs-CRP and normal LDL cholesterol is cost-effective for those with Framingham risk score ≥10%.73,74 However, others argue that it is more cost-effective to begin statin therapy without assessing hs-CRP, on the assumption that the drug is safe and is beneficial even in patients with normal CRP.75
It is important to note that the population of the JUPITER trial, although apparently healthy, all had at least one cardiovascular risk factor, such as obesity or smoking. According to Rashid,76 the JUPITER results warrant further LDL cholesterol lowering than is currently targeted in primary prevention groups that have a pre-existing condition or lifestyle that elevates cardiovascular risk but still do not have a high global CVD risk as assessed with current algorithms. Lifestyle modifications (smoking cessation, normalization of body weight and dietary changes) should be achieved first before considering statin therapy. Assessment of hs-CRP can help identify this patient subgroup, who should begin preventive therapy early in an attempt to reduce the prevalence of cardiovascular disease.
With regard to secondary prevention, the findings of the Cholesterol And Recurrent Events (CARE) trial, a randomized study assessing the effect of pravastatin after MI, showed that although the relative risk of adverse coronary events was substantially reduced with statin therapy in patients with and without evidence of inflammation, the reduction was greater in those with evidence of inflammation as assessed by hs-CRP measurement (54% vs. 25%), even though lipid levels were similar in the two groups.48 This suggests that statins are particularly effective in patients with elevated hs-CRP. The PROVE-IT (Pravastatin or Atorvastatin Evaluation and Infection Therapy) study demonstrated that intensive statin therapy reduces hs-CRP levels to less than 2mg/l, resulting in lower risk of MI and fatal coronary events, independently of reductions in LDL cholesterol (Figure 3).77 A subanalysis of the Aggrastat-to-Zocor study showed that hs-CRP levels 30 days and four months after MI are independently associated with long-term survival and that more aggressive statin therapy is likely to result in low CRP.78 The evidence in these studies of the pleiotropic effects of statins suggests that assessment of CRP levels can identify individuals who do not have elevated LDL cholesterol but nonetheless would benefit from statin therapy to reduce cardiovascular events (Table 3).
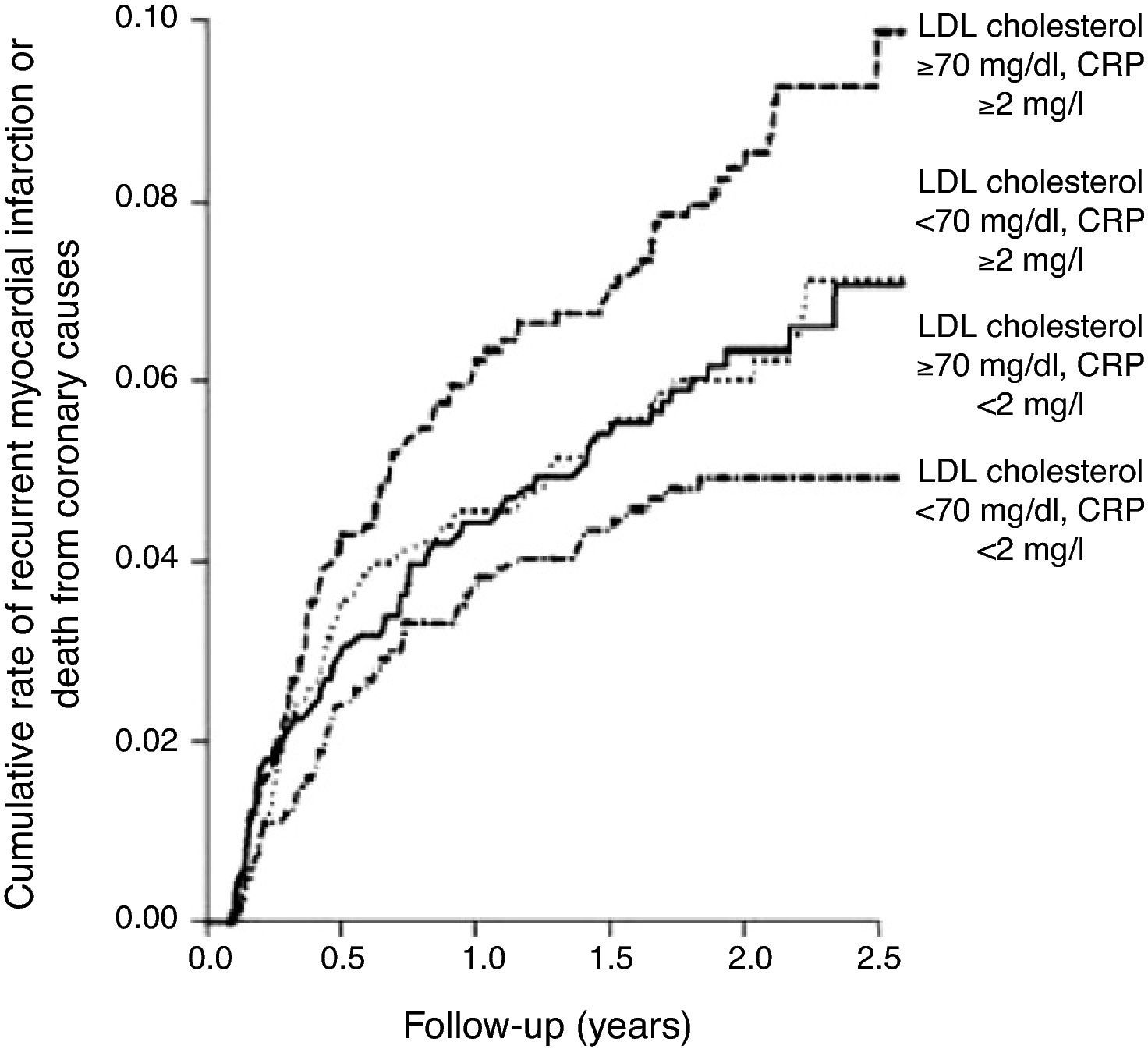
Intensive pravastatin therapy in patients with acute coronary syndrome reduced high-sensitivity C-reactive protein to below 2mg/l, resulting in reduced risk of myocardial infarction and fatal coronary events, independently of reductions in LDL cholesterol.
In the Physician's Health Study, the use of aspirin was associated with a significantly larger reduction in risk of MI in men in the highest quartile of hs-CRP levels than in those in the lowest quartile (55.7% vs. 13.9%).16 However, few studies have assessed the direct effect of aspirin on CRP levels; one small randomized trial studied the effect of low-dose aspirin in healthy volunteers but did not detect any effect on CRP.79
Variability in hs-CRP levelsVarious groups have addressed the question of short-term fluctuations (15 days-6 months) in hs-CRP levels in clinically stable individuals. Studies have been performed in patients with stable CAD,80,81 patients under aggressive statin therapy81 and healthy individuals82–85; their conclusions are that hs-CRP variability is independent of clinical events, medication, body mass index and smoking, is the same in men and women, and is age-related.80,86,67 Intraindividual variability was 42–63% in healthy volunteers84 and 1.79mg/l (95% CI: 1.60–2.00) in patients with stable CAD,81 and was not mirrored by variations in other measures of inflammation.81
These findings suggest that there may be practical limitations to the use of this biomarker, particularly for predicting cardiovascular risk. Some authors therefore recommend that risk for CAD should be determined solely on the basis of conventional risk factors.28
Current guidelinesIn 2003, the American Heart Association and the US Centers for Disease Control and Prevention published guidelines on the use of markers of inflammation in cardiovascular risk assessment,87 and in 2009 the National Academy of Clinical Biochemistry published guidelines on emerging biomarkers for primary prevention of cardiovascular disease.88
According to these guidelines, hs-CRP should not be measured in the general population to determine cardiovascular risk, but can be used in risk stratification of adults at intermediate risk for CAD (10–20% risk at 10 years), to help decide whether to begin primary prevention with statins. hs-CRP levels should be expressed in mg/l and patients should be classified as low risk (<1.0mg/l), intermediate risk (1.0–3.0mg/l), or high risk (>3.0mg/l). If the concentration is <3mg/l, measurement does not need to be repeated. If the value is >3mg/l, it should be repeated at least two weeks later when there is no evidence of active systemic inflammation; the lower of the two results should be used. Values of >10mg/l suggest a very strong acute phase response and, if not of cardiovascular cause, require further etiological investigation.
Therapy (statins or aspirin) based on hs-CRP levels should be at the discretion of the clinician, since its benefit is still uncertain, and little evidence supports the use of serial testing for hs-CRP as a means to monitor therapy in primary prevention. Individuals with persistently high levels should improve their lifestyles (e.g. weight loss, regular exercise, dietary modification and smoking cessation), irrespective of their LDL cholesterol levels.
In 2009, the Canadian Cardiovascular Society also published new guidelines on primary cardiovascular prevention,89 which recommend that in individuals with intermediate cardiovascular risk according to conventional risk scores, hs-CRP should be assessed as well as LDL and HDL cholesterol in order to improve risk stratification. The European Atherosclerosis Society has yet to pronounce on this issue. By contrast, the 2007 European guidelines on cardiovascular disease prevention state that incorporation of CRP and other emerging risk factors into prediction of cardiovascular risk may be premature and is therefore not recommended.90
In February 2010, the US Food and Drug Administration approved rosuvastatin for prevention of cardiovascular events in women aged over 60 and in men aged over 50 with hs-CRP >2mg/l and another conventional risk factor, even without hyperlipidemia.91
Both European and American guidelines consider that in patients with documented CAD hs-CRP measurement may be useful as an independent marker for assessing likelihood of death, MI or restenosis after PCI.87,92 However, secondary preventive interventions and application of ACS treatment guidelines should not be dependent on hs-CRP levels.
It should be noted that in 2010, a study by Hemingway et al. evaluating the quality of research into the prognostic value of CRP in stable CAD concluded that the 83 studies analyzed suffered from a variety of biases and that any link between hs-CRP and prognosis is so weak that it cannot be used as the basis for clinical recommendations.93
ConclusionThere is growing evidence that hs-CRP is an important marker of cardiovascular risk and is linked to the pathophysiology of atherosclerosis, providing additional value in primary and secondary prevention. Despite the limitations to its use in routine clinical practice, particularly interindividual variability, the available data indicate that selective determination of hs-CRP is useful in individuals with intermediate cardiovascular risk (10–20% risk at 10 years) in order to optimize risk stratification and clinical management.
Ethics disclosuresProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the responsible Clinical Research Ethics Committee and in accordance with those of the World Medical Association and the Helsinki Declaration.
Right to privacy and informed consentThe authors must have obtained the informed consent of the patients and/or subjects mentioned in the article. The author for correspondence must be in possession of this document.
Conflict of interestsThe authors have no conflicts of interest to declare.
Please cite this article as: Silva D. Proteína C reactiva de alta sensibilidade como biomarcador de risco na doença coronária. Rev Port Cardiol 2012. http://dx.doi.org/10.1016/j.repc.2012.02.018.
