






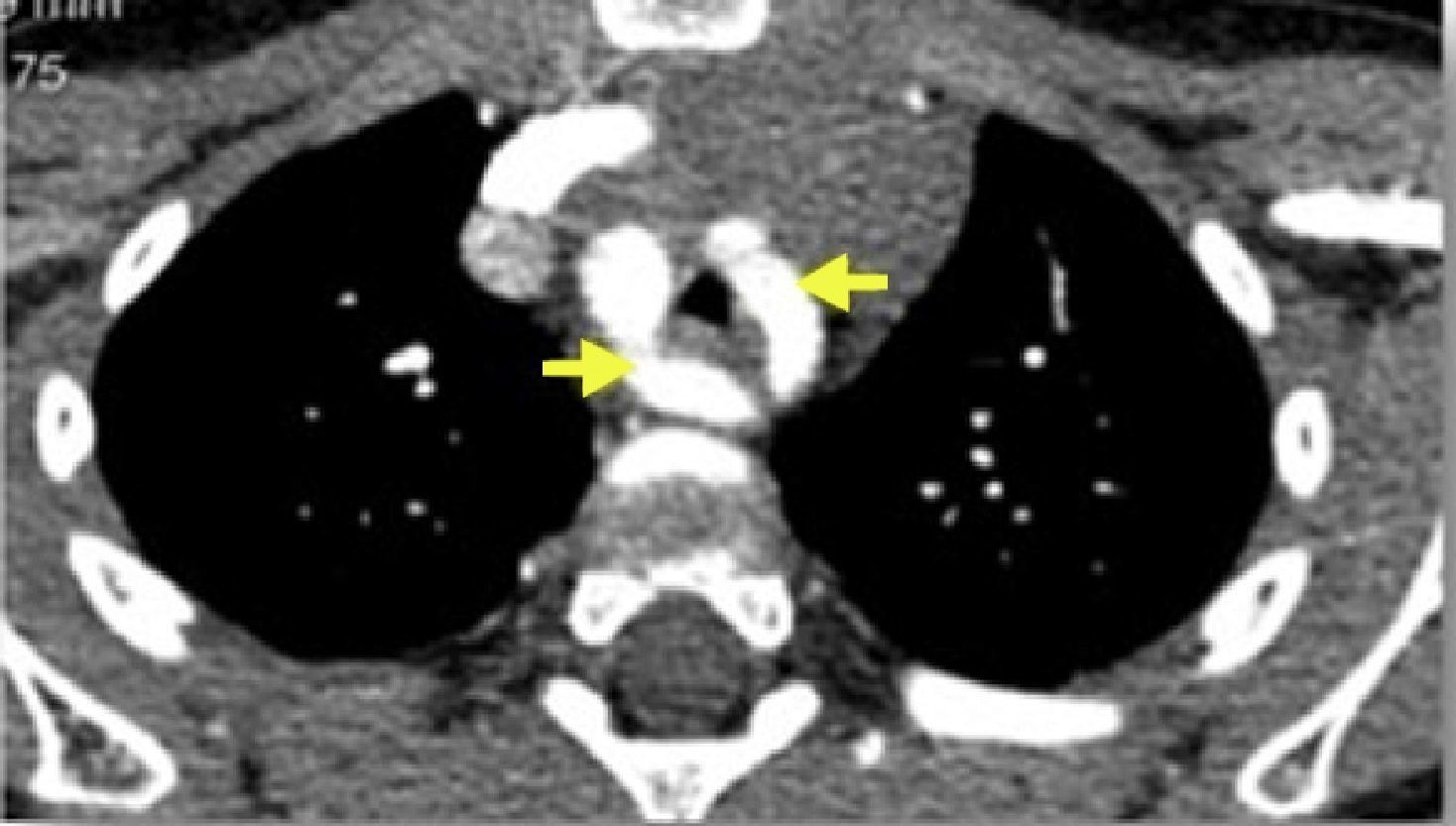
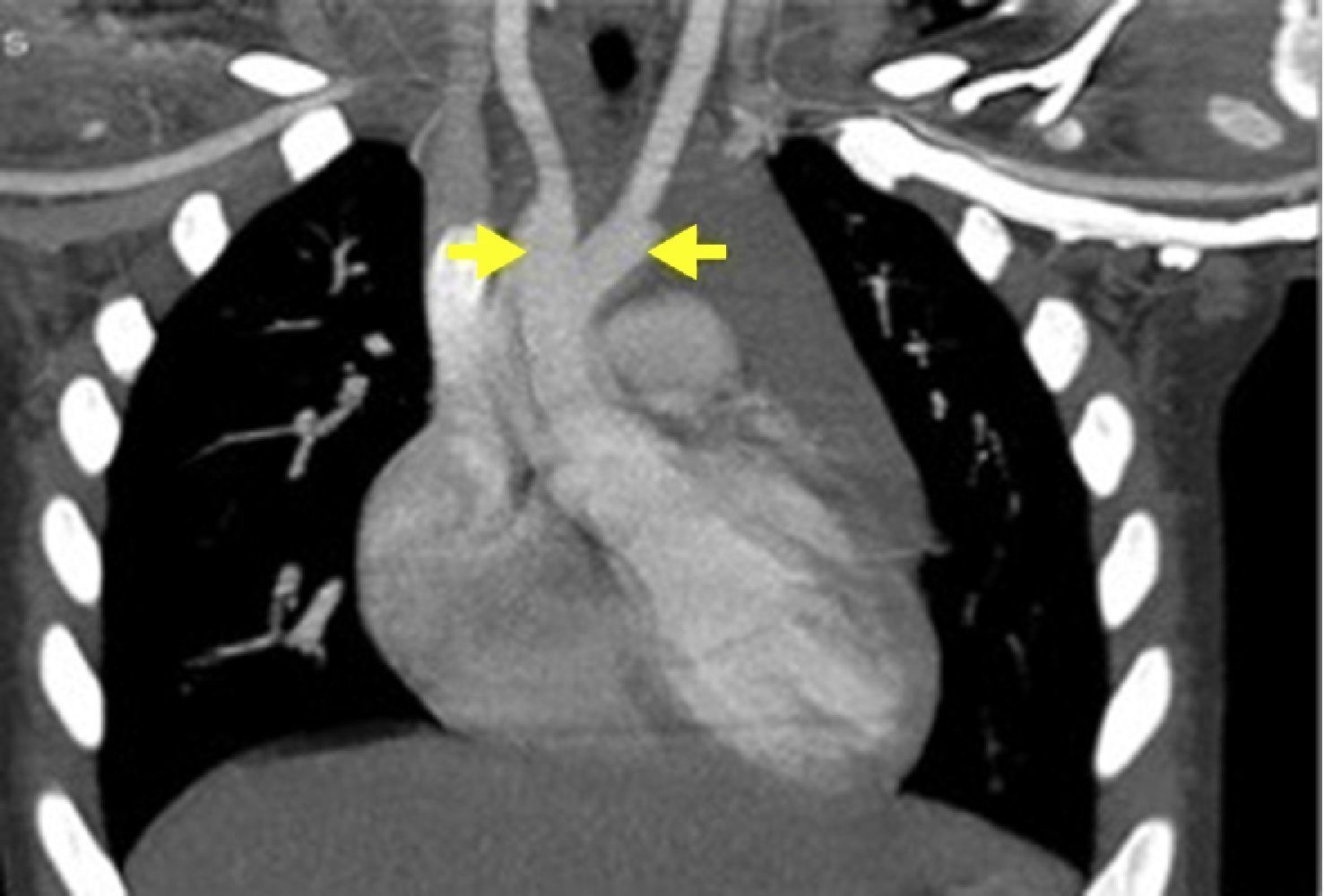
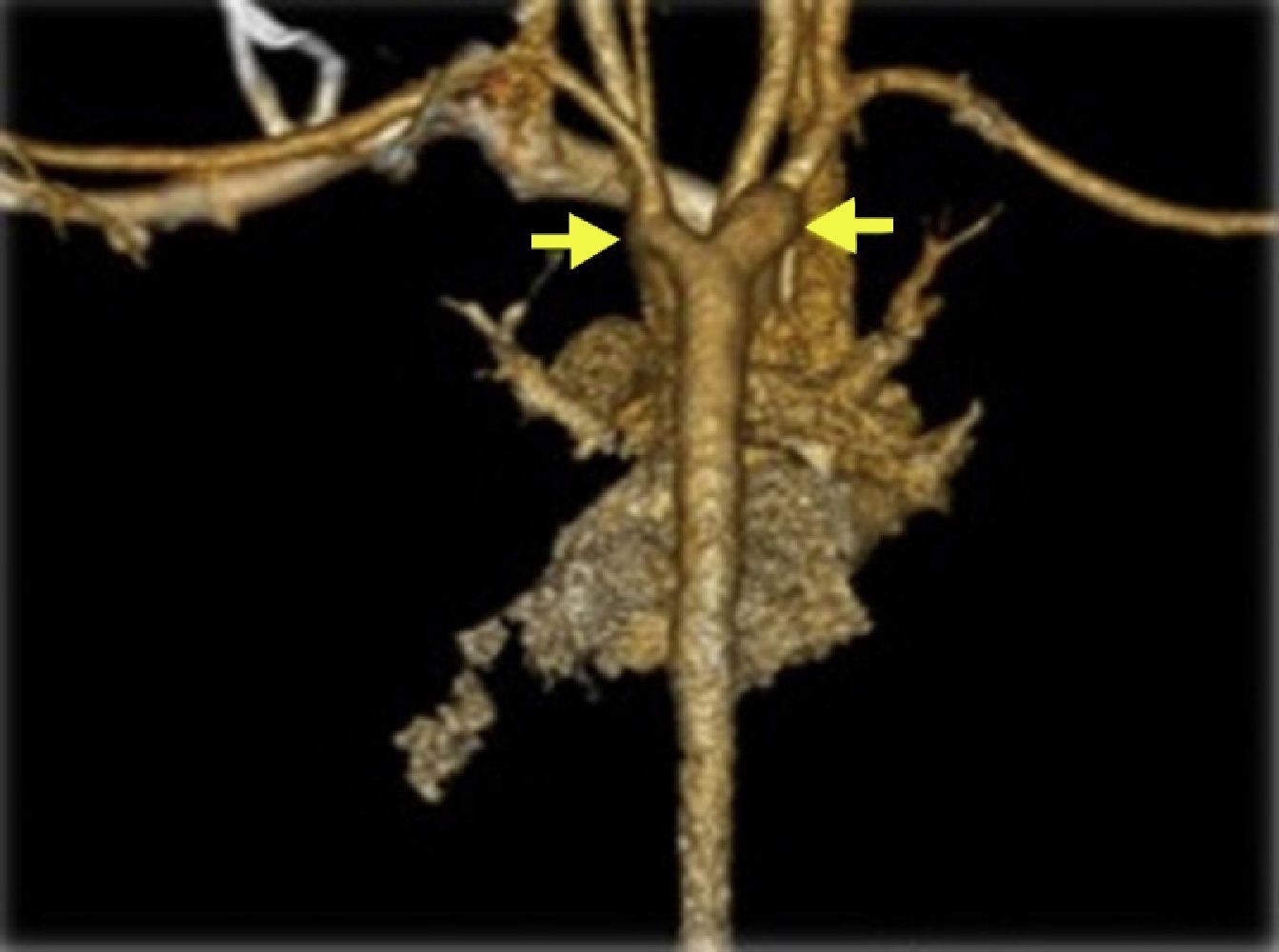
A boy aged 2.5 years presented biphasic stridor at three months of age, which worsened with crying, feeding and upper respiratory tract infections. Fiberoptic bronchoscopy (FOB) at five months diagnosed tracheomalacia, with 80% dynamic collapse of the lower two-thirds of the trachea. The child had normal growth and no difficulty feeding. FOB at 21 months due to persistent stridor showed marked dynamic collapse and extrinsic compression of the trachea. Thoracic computed tomography (angio-CT) angiography identified a vascular ring due to a double aortic arch (Figures 1–3), causing extrinsic compression of the trachea with marked reduction in its caliber (Figure 4). There were no other cardiac malformations on echocardiographic study. At 23 months the child underwent ligation and division of the more hypoplastic arch (left anterior) by thoracotomy. The postoperative course was good, and the child currently has mild stridor only.

Vascular rings account for 1% of congenital heart defects and are the most common malformation causing airway compression. In this case, the clinical presentation dictated the sequence of imaging exams – FOB followed by angio-CT. This combination of imaging techniques is essential for preoperative assessment. angio-CT angiography provides better spatial and temporal resolution, rapid image acquisition requiring only sedation or brief anesthesia in uncooperative patients, and three-dimensional image reconstruction, and is thus the preferred imaging modality, especially with the lower radiation levels required with modern equipment. Assessment of tracheomalacia or other airway dysfunction still requires video bronchoscopy.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of dataThe authors declare that no patient data appears in this article.
Right to privacy and informed consentThe authors declare that no patient data appears in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Sanches B, Rebelo D, Brito S, et al. Duplo arco aórtico na origem de estridor persistente: sequência de imagens para orientação cirúrgica. Rev Port Cardiol. 2015;34:629–630.
