




Abnormalities of the papillary muscle (PM) are a rare disorder that has been described in patients with hypertrophic cardiomyopathy1–3 or cardiac amyloidosis causing significant left ventricular outflow tract (LVOT) obstruction. These anomalies are often challenging to diagnose with 2D echocardiography, and real-time 3D echocardiography (RT3D) facilitates the diagnosis by providing accurate imaging and delineation of the spatial relationship between the cardiac structures.
Case reportA 43-year-old black African woman, asymptomatic at presentation (blood pressure 105/71mmHg, heart rate 82bpm, body surface area 1.52m2), diagnosed with sickle cell disease, was investigated for pulmonary hypertension in our department. Echocardiography was requested for the assessment of cardiac function and estimation of pulmonary artery pressures.
Full 2D and 3D transthoracic echocardiography (TTE) was performed and 3D images were acquired and analyzed using Philips Qlab offline analysis software. The echocardiogram revealed a dilated left ventricle (LV) with normal wall thickness and good global systolic function.
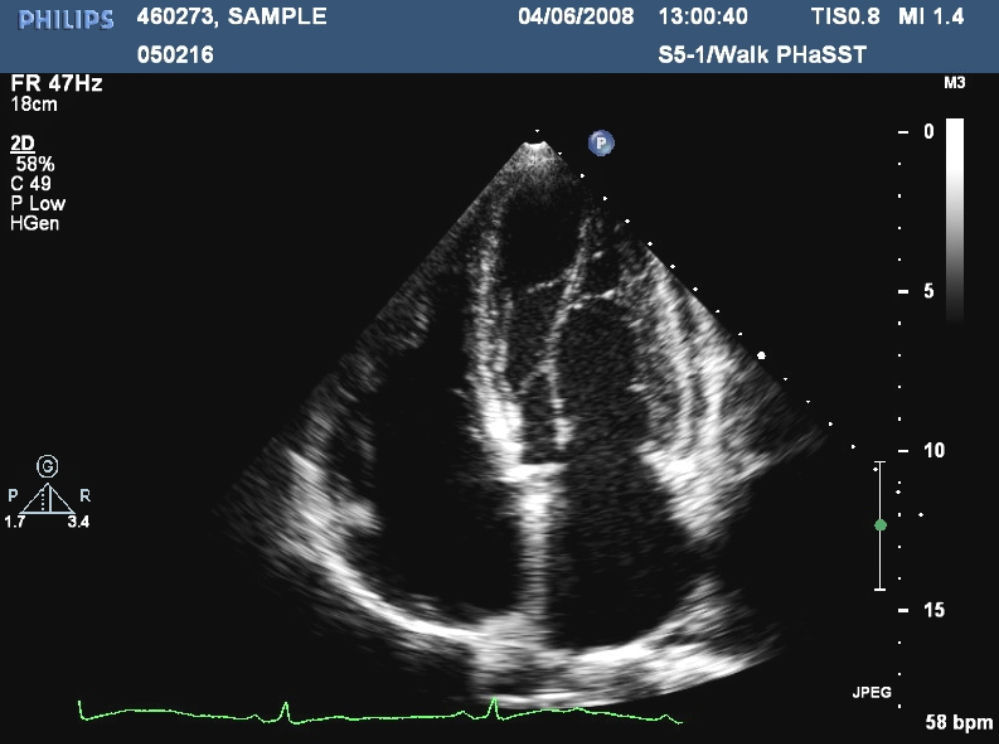
In parasternal long-axis 2D view, the anterolateral PM appeared in an unusual position, and in short-axis view and apical 4 chambers view (Figure 1) it was clearly inserted lower than normal. A complete Doppler assessment revealed no high velocity or turbulent flow pattern and no significant LVOT or intracavitary gradient was identified.
3D echocardiography clearly showed the lower insertion of the PM and the hypertrophied chordae (Figure 2). A follow-up echocardiography study was recommended to assess left ventricular hypertrophy but the patient died a few months later due to a subarachnoid hemorrhage. No post-mortem was performed.
Discussion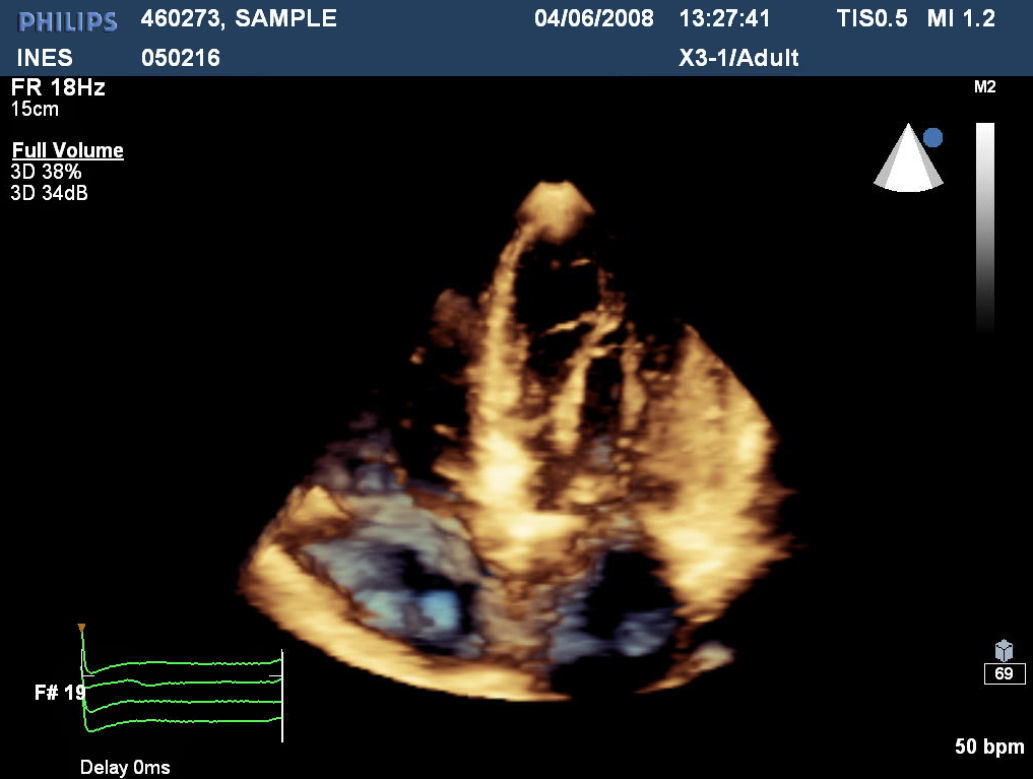
Anomalous insertion of PMs not causing LVOT obstruction is a rare abnormality.1–4 RT3D is being increasingly used in the clinical setting to accurately identify cardiac structures and anatomy.5,6 Its role is mainly in providing additional spatial information to 2D TTE in the identification of complex anatomic structures. The normal variant of low insertion of the anterolateral PM without LVOT obstruction may be observed in healthy individuals but an association with sickle cell disease cannot be excluded; further investigations are needed to confirm this association. To our knowledge, this is the first case in sickle cell disease of an anomalous insertion of PMs not causing LVOT obstruction reported in the literature.
Ethical disclosuresConfidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data and that all the patients included in the study have received sufficient information and have given their informed consent in writing to participate in the study.
Right to privacy and informed consentThe authors have obtained the informed consent of the patients and/or subjects mentioned in the article. The author for correspondence is in possession of this document.
Protection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this investigation.
Conflicts of interestThe authors have no conflicts of interest to declare.
