





Congenital anomalies of the coronary arteries are uncommon and can present a diagnostic challenge.
The authors present the case of a patient with recurrent chest pain during exertion admitted for acute coronary syndrome. Coronary angiography revealed no coronary lesions but showed that the right coronary artery originated from the anterolateral aortic wall, above the sinuses of Valsalva, leading to suspicion of compression by the pulmonary artery, confirmed by CT angiography. The patient underwent surgical revascularization with a good result.
The authors highlight the need to consider compression of an anomalous coronary artery by the pulmonary artery in the differential diagnosis of recurrent chest pain on exertion and acute myocardial infarction without significant coronary stenosis.
A origem anómala das artérias coronárias é um achado pouco comum e que pode constituir um desafio diagnóstico.
Apresenta‐se o caso clínico de uma doente com dor torácica recorrente durante o esforço, admitida com síndrome coronária aguda e cuja coronariografia não revelou lesões coronárias epicárdicas. Foi constatada origem da coronária direita na parede ântero‐lateral esquerda da aorta, acima dos seios de Valsalva, revelando a origem anómala dessa artéria e potencial compressão pela artéria pulmonar, o que foi confirmado por angio‐TC. A doente foi submetida a revascularização cirúrgica, com bom resultado.
Os autores salientam a necessidade de incluir a potencial compressão de coronárias com origem anómala pela artéria pulmonar, no diagnóstico diferencial da dor torácica recorrente com o esforço e enfarte agudo do miocárdio sem estenoses coronárias significativas.
Congenital anomalies of the coronary arteries are found in 0.2–1.2% of the general population.1 Most patients with anomalous origin of a coronary artery are asymptomatic and diagnosis is often an incidental finding on coronary angiography or computed tomography (CT). Its clinical significance depends on various factors, including the artery's origin and course and the area of myocardium perfused. When present, symptoms are the result of myocardial ischemia and can include angina, arrhythmia, syncope, myocardial infarction or sudden death; diagnosis is essential for appropriate treatment.
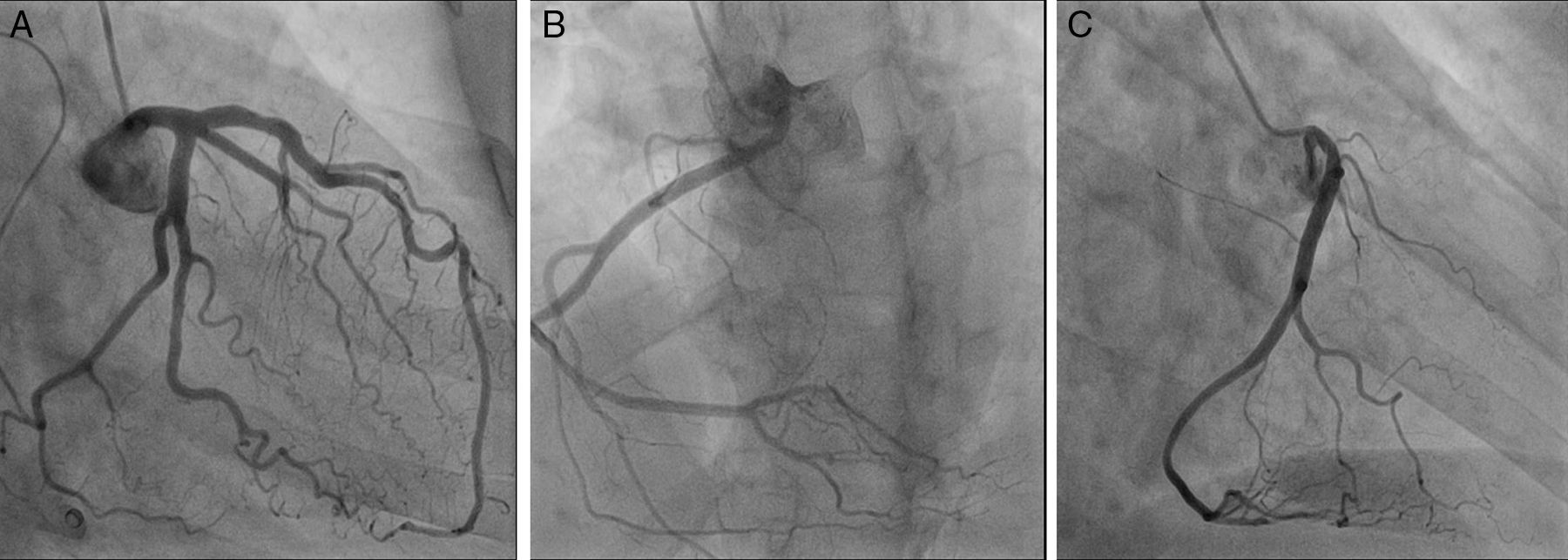
Case reportA 56‐year‐old woman, with a history of hypertension, hypothyroidism and anxiety attacks, was seen in the emergency department for constricting chest pain, non‐radiating, and dyspnea, that began during a water exercise session and subsided after 20 minutes’ rest. She reported similar episodes in the past but of shorter duration, always triggered by exercise, particularly swimming. The electrocardiogram revealed no significant alterations, but laboratory tests showed slight elevation of myocardial necrosis markers. The patient was admitted with a diagnosis of non‐ST elevation acute coronary syndrome. Transthoracic echocardiography revealed good biventricular systolic function, with no regional wall motion abnormalities. Cardiac catheterization showed right dominance, no significant stenosis, and the right coronary artery (RCA) originating from the lateral wall of the ascending aorta, above the sinuses of Valsalva (Figure 1), potentially being compressed between the aorta and the pulmonary artery. Exercise testing documented ischemia (Figure 2A). Coronary CT angiography revealed the RCA originating between the left anterolateral aortic wall and the ascending portion of the pulmonary artery, its proximal segment describing a convoluted course parallel to the aorta and close to the pulmonary artery (Figure 3). The patient was diagnosed with myocardial ischemia due to anomalous origin of the RCA and was referred for surgical revascularization. While awaiting surgery, she continued to suffer recurrent anginal episodes despite optimal anti‐ischemia therapy. Surgical inspection confirmed that the RCA originated in the left anterolateral wall of the ascending aorta, above the sinuses of Valsalva, with an extramural and interarterial course, and latero‐lateral anastomosis of the RCA to the anterior aortic wall was performed (Figure 4A). Postoperative exercise testing documented no ischemia (Figure 2B). Repeat coronary CT angiography (Figure 4B and C) showed a good surgical result. Fifteen months after surgery, the patient is asymptomatic, with no recurrence of angina.
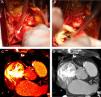
Coronary angiography: (A) (right anterior oblique 30°; caudal 20°) showing the left coronary artery with no epicardial lesions; (B) (left anterior oblique 20°; cranial 20°) and (C) (right anterior oblique 30°) showing the right coronary artery with no epicardial lesions, originating in the left anterolateral aortic wall, above the sinuses of Valsalva.
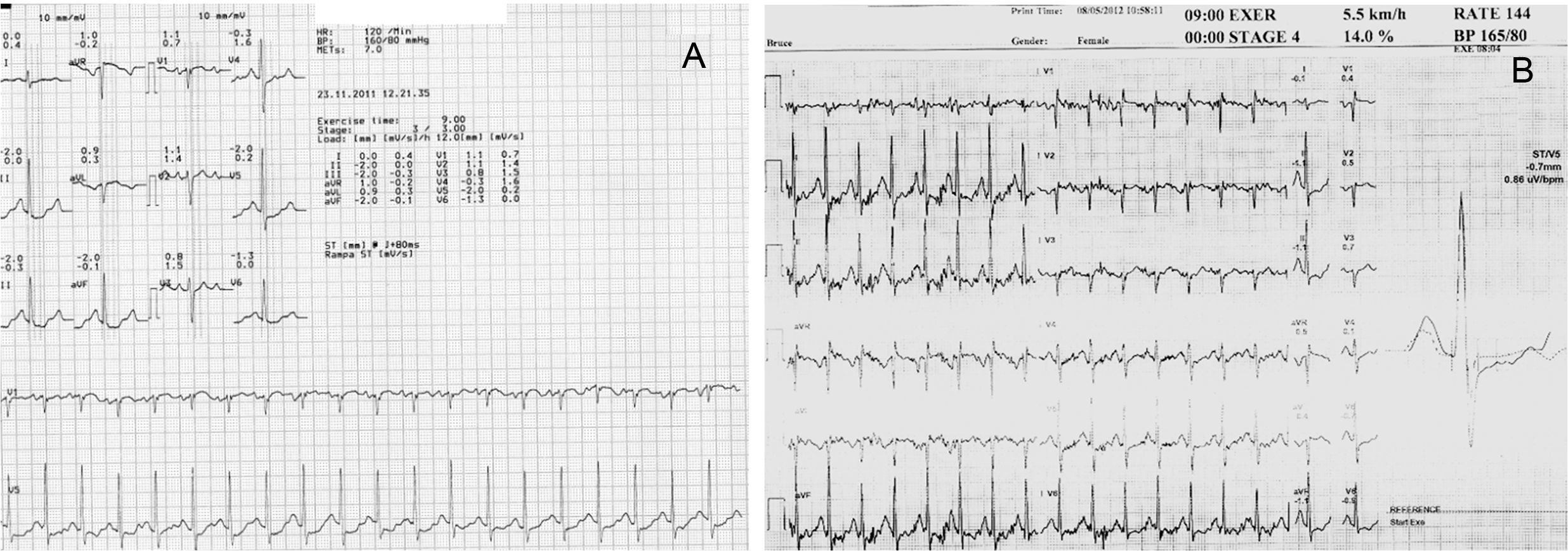
Multislice computed tomography: (A) and (B): three‐dimensional volume‐rendered image showing origin of the right coronary artery from the left anterolateral aortic wall, above the sinus of Valsalva, with an initial course between the aorta and the ascending portion of the pulmonary artery; (C), (D) and (E): multiplanar reconstruction images showing extramural and interarterial course of the right coronary artery. LM: left main; Pulmonary ASC: pulmonary artery; RCA: right coronary artery.
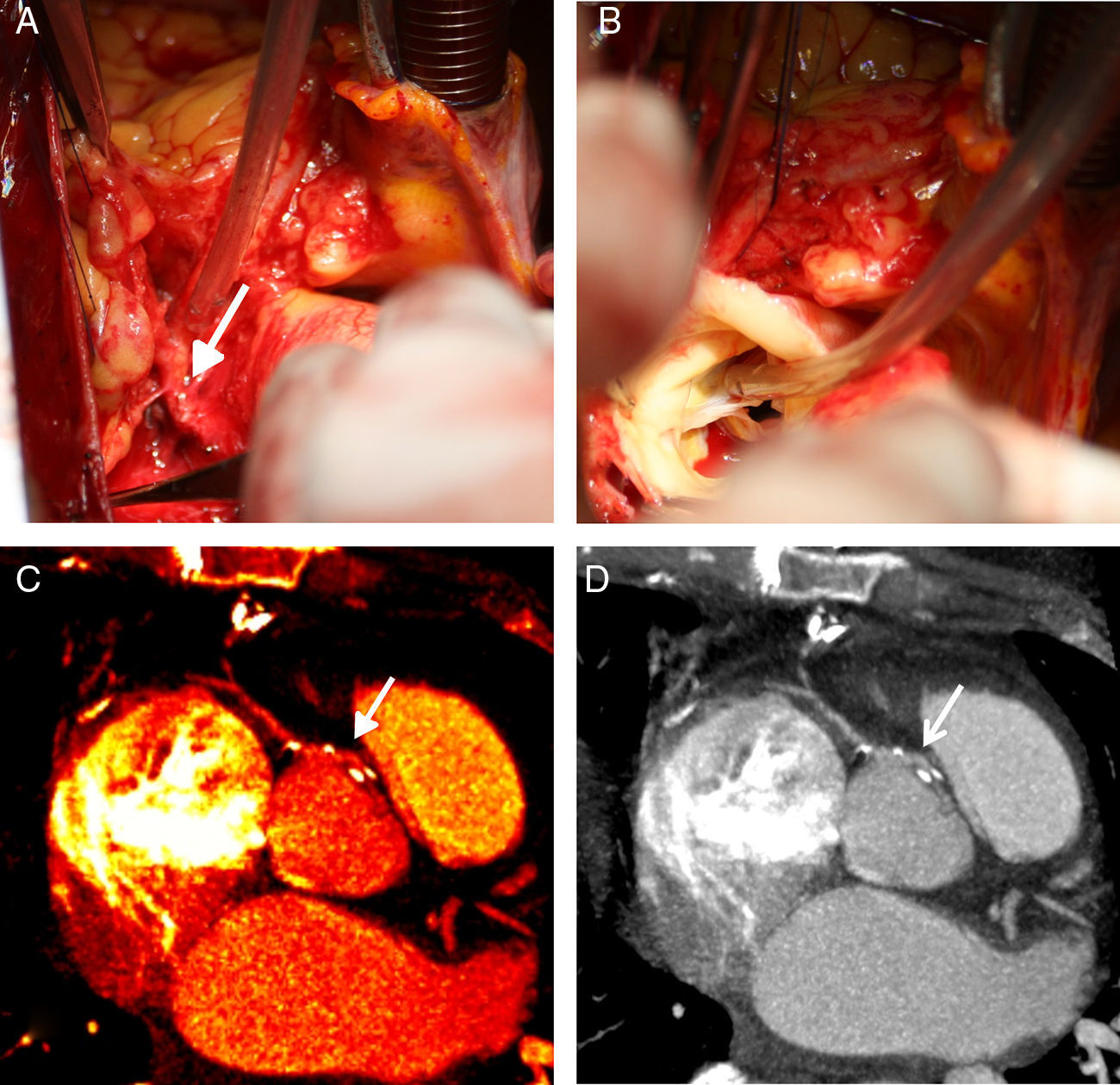
(A): Surgical dissection of the emergence of the right coronary artery showing its origin in the left anterolateral aortic wall and an extramural and interarterial course; (B): following transection of the aorta, the origin is shown to be above the sinus of Valsalva, posterior to the commissure separating the right and left cuspids (note the angle of the coronary ostium); (C) and (D): multislice computed tomography multiplanar reconstruction following surgical revascularization, showing latero‐lateral anastomosis (arrows). The high‐density images correspond to surgical clips.
Various criteria have been used to classify normal and anomalous coronary arteries. The system proposed by Angelini in 1988 includes nomenclature and definitions of both normal variations and anomalous coronary arteries.
Anomalous origin of the RCA is a rare congenital anomaly.2 In most cases, the RCA originates in one of two locations: the left coronary sinus or the anterior aortic wall, above the coronary sinus.3 These anomalies have no clinical significance in most patients, but they can be associated with considerable morbidity or even sudden death.4 The mechanism underlying myocardial ischemia is primarily dynamic obstruction, possible causes being ostial obstruction due to the acute angle between the ostium and the artery, compression of the RCA between the aorta and the pulmonary artery, and elongation of the RCA due to aortic or pulmonary artery dilatation.2
Preoperative evaluation of coronary anatomy and its relation to surrounding structures is extremely important to provide an accurate assessment of the anomaly and to help plan the repair. The method of choice to assess these patients is multislice CT angiography, which allows three‐dimensional visualization of the coronary arteries with high spatial resolution.5
Recent years have seen progressive developments in the surgical techniques used to treat coronary artery anomalies requiring intervention, of which the most common are coronary artery fistulas and anomalous origin from the pulmonary artery or the aorta.6 The choice of surgical intervention for each type of coronary anomaly depends on several anatomical, physiological and patient‐dependent variables. Despite advances in techniques and improved outcomes, there is still disagreement as to the most appropriate treatment for these patients.
In cases of anomalous origin of the RCA from the anterior wall of the aorta, or as in our patient the lateral wall, with an extramural and interarterial course between the aorta and the pulmonary artery, there are various surgical options, including reimplantation of the ostium and coronary artery bypass surgery using a mammary artery or saphenous vein graft, with or without ligation of the anomalous artery.6 The goal of intervention is to provide reliable perfusion to the anomalous arterial system downstream of the site(s) of potential obstruction. The choice of approach will depend on the patient's anatomy and whether reimplantation of the coronary ostium is possible. If the anatomy is favorable, then reimplantation of the ostium is an appropriate procedure; otherwise, coronary bypass surgery using a mammary artery or saphenous vein graft is the best option, although there is still disagreement concerning the use of mammary artery or saphenous vein grafts, given the greater long‐term patency but higher risk of occlusion of arterial grafts used to bypass vessels with competitive flow.6–8 Good results have been reported with both reimplantation of the ostium and bypass surgery.6 Another decision to be made is whether to ligate a patent anomalous artery in order to eliminate competitive flow.6
Another treatment option is percutaneous coronary intervention (PCI), but it is a difficult procedure, requiring appropriate hardware selection and a high level of operator skill and experience.9 There have been cases of good long‐term outcomes with PCI but others have reported complications, such as procedure failure with need for urgent bypass surgery, and stent fracture.9,10
In the present case, given the high origin and extramural course of the RCA (Figure 4A), reimplantation would have resulted in an acute angle in its initial course or an even higher abnormal implantation; it was thus decided to perform latero‐lateral anastomosis to the anterior aortic wall, with good clinical results and ischemia test.
The prognostic impact of coronary artery anomalies varies depending on the artery involved; if the left coronary artery originates in the right sinus of Valsalva the risk of sudden death is significantly higher than if the RCA arises in the left coronary sinus, which should be borne in mind when deciding on the approach to adopt.11,12
ConclusionThis case illustrates the importance of clinical suspicion of anomalies of coronary origin in patients with recurrent angina and no evidence of epicardial coronary disease. It also highlights the role of CT angiography in patients with anginal symptoms and anomalous origin of the RCA from the anterior or lateral aortic wall, above the sinuses of Valsalva. Surgical revascularization is one treatment option, with good long‐term outcome.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data and that all the patients included in the study received sufficient information and gave their written informed consent to participate in the study.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Vieira C, Nabais S, Salgado A, et al. Origem coronária anómala: da suspeita à revascularização cirúrgica. Rev Port Cardiol 2014;33:53.
