



We report the case of a young man who accidentally received a prolonged electric discharge from electrical wires and released the electric source with the help of an inappropriate shock from his implantable cardioverter-defibrillator (ICD), after misinterpretation of the electrical signal by the device as a ventricular tachycardia. This case illustrates the “electrical noise” phenomenon, and underscores the need for precautions for patients with an ICD and their physicians.
Relatamos o caso de um jovem que acidentalmente recebeu uma descarga eléctrica prolongada por contacto com fios eletrónicos. Foi ajudado a libertar a fonte elétrica pela administração inapropriada de um choque pelo cardioversor desfibrilador implantável (CDI), depois de uma interpretação errada do sinal elétrico pelo dispositivo, lido como uma taquicardia ventricular. Este caso ilustra o fenómeno de «ruído elétrico», e sublinha as precauções necessárias para os doentes portadores de CDI e para os seus médicos.
We report the case of a 36-year-old male with arrhythmogenic right ventricular cardiomyopathy and an implantable cardioverter-defibrillator (ICD) since 2007 for primary prevention of sudden cardiac death. While abroad on holiday, the patient received an electric discharge while manipulating computer wires. On his return two weeks later, he made an appointment at our pacemaker clinic in order to confirm the proper functioning of his device. The patient had not sought medical assistance in the meantime, and denied any cutaneous or other lesion related to the event.
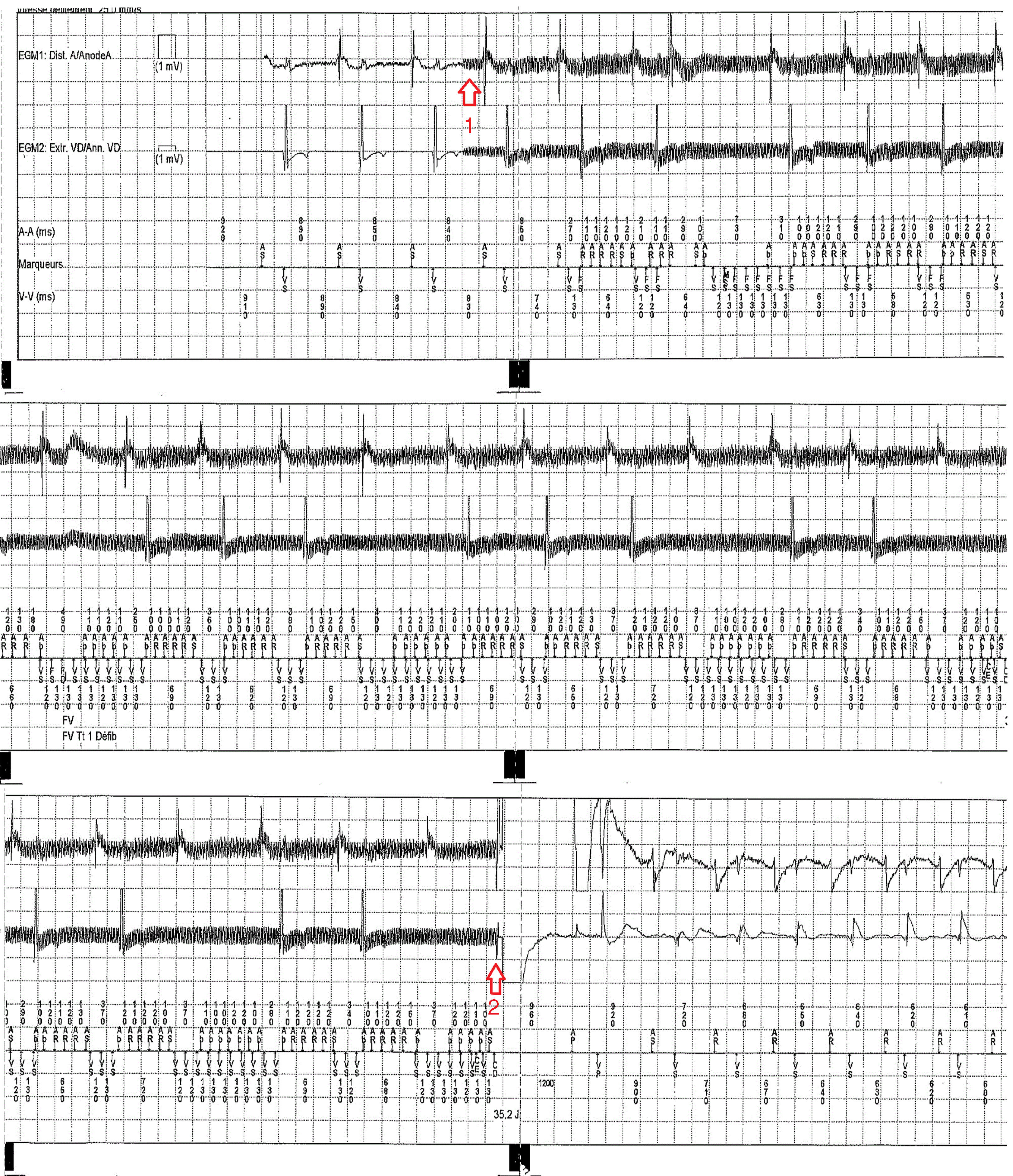
ICD interrogation revealed the application of a shock 11 seconds after the beginning of continuous high-frequency electrical activity, interpreted as an episode of ventricular tachyarrhythmia by the device.
The review of the ICD electrogram (Figure 1) clearly shows atrioventricular activity with narrow and regular QRS complexes parasitized by high-frequency low-intensity baseline interference, corresponding to the accidental 50–60 Hz electrical exposure, terminated by the ICD shock delivery. Unlike the case reported by Saguner and Duru1 in which a shock was avoided by appropriate detection of interference by the ICD's noise reversion algorithm, our patient's device was not equipped with this functionality, and hence was unable to respond adequately, delivering a 35-J shock that probably helped the patient release the electrical source, as noise termination occurred immediately after shock delivery and as the patient himself reported.
This case highlights a rare situation in which an inappropriate shock can be beneficial and underscores the importance of advising patients carrying a defibrillator to avoid any electrical exposure.2,3
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
