
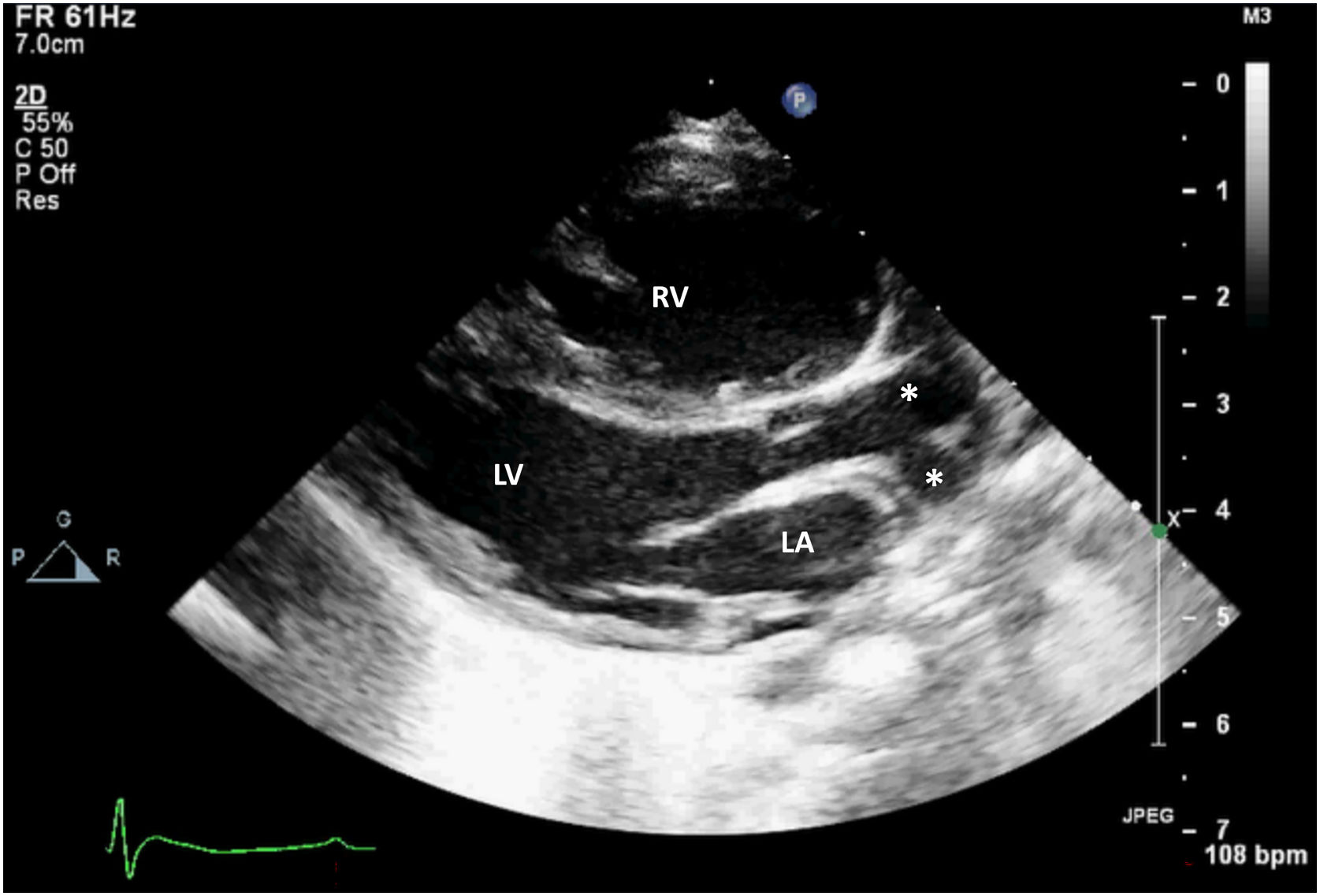
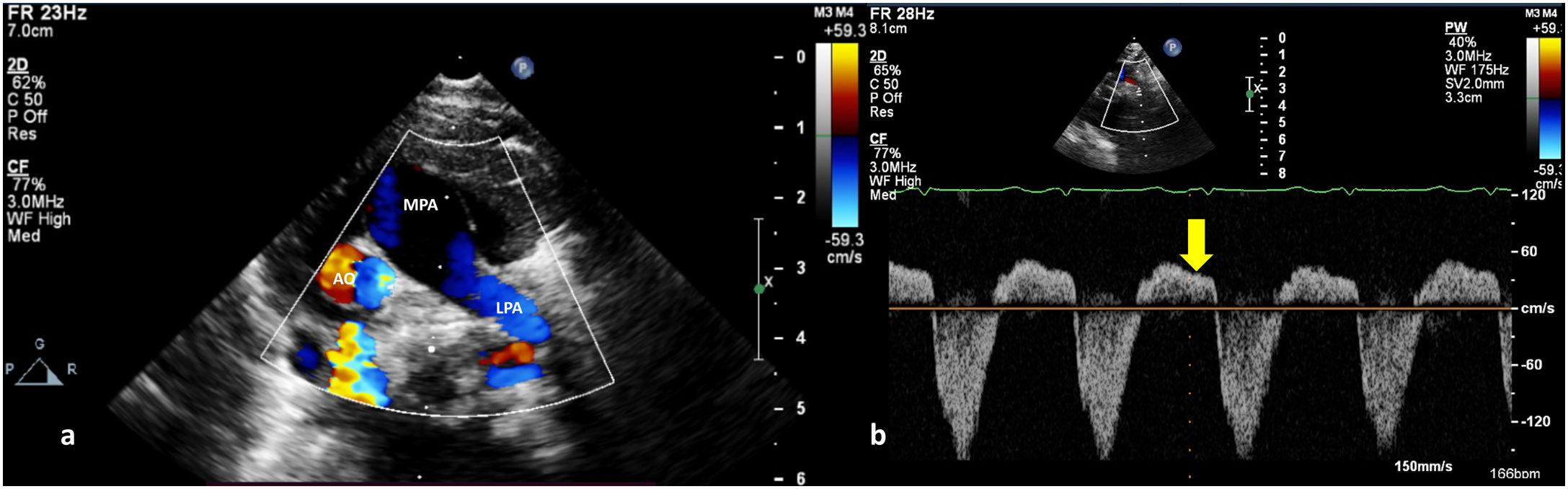
A 10-day-old term neonate with tachypnea and peripheral oxygen saturation of 90% was referred to us with a diagnosis of transposition of the great arteries with intact ventricular septum for early arterial switch operation. The child weighed 2.8 kg and was not dysmorphic. Precordial examination revealed cardiomegaly, loud second sound and a grade 2 mid-systolic murmur in the upper left sternal border. Clinical examination and transthoracic echocardiography suggested usual arrangement of the visceroatrial structures and normal leftward cardiac apex. Systemic and pulmonary venous drainage were normal. A stretched open foramen ovale shunted right-to-left. The atrioventricular relationship was concordant. The parasternal long-axis view showed intact interventricular septum, good left ventricular function and a bifurcating great artery arising from the left ventricle (Figure 1 and Video 1). The great artery relationship was noted to be normal with an unobstructed anterior and leftward located main pulmonary artery. The right pulmonary artery was not seen to arise from the main pulmonary artery, unlike the left pulmonary artery (Figure 2a). The anomalous origin of the right pulmonary artery from the ascending aorta gave the appearance of bifurcation. Pan-diastolic flow reversal in the descending aorta was confirmative of the aortic runoff (Figure 2b). The arterial duct was not patent. The right ventricle was dilated and dysfunctional. The estimated left pulmonary artery systolic pressure was 105 mmHg from the tricuspid regurgitation jet.
. LA: left atrium; LV: left ventricle; RV: right ventricle.")
 Transthoracic color Doppler echocardiographic still, parasternal short-axis projection, showing the main pulmonary artery (MPA) continuing as left pulmonary artery (LPA) and (b) pulsed wave Doppler from the descending aorta showing pandiastolic flow reversal (yellow arrow). AO: aortic valve.")
(a) Transthoracic color Doppler echocardiographic still, parasternal short-axis projection, showing the main pulmonary artery (MPA) continuing as left pulmonary artery (LPA) and (b) pulsed wave Doppler from the descending aorta showing pandiastolic flow reversal (yellow arrow). AO: aortic valve.
Careful echocardiographic assessment is crucial to distinguish isolated right pulmonary artery from the aorta with severe pulmonary hypertension from transposition. Hemitruncus is primarily an acyanotic congenital heart disease, with two separate semilunar valves. However, a stretched open foramen ovale may cause systemic desaturation following right ventricular dysfunction and advanced heart failure in hemitruncus. Reimplantation of the right pulmonary artery is curative.
Ethical considerationsThe study was conducted in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its amendments. Written informed consent was obtained from the parent of the patient concerned. No patient identity particulars have been disclosed.
Authors’ contributionsConcept, data collection, and drafting article – AGK. AGK, WRS, DS, HKN, KMK critically reviewed the manuscript. All authors approved the final version.
FundingNone declared.
Conflict of interestsThe authors have no conflicts of interest to declare.
The following are the supplementary data to this article:
Transthoracic two-dimensional echocardiography cine loop, parasternal long-axis projection, with color comparison, showing the bifurcating great artery arising from the left ventricle (white asterisk: aorta, yellow asterisk: right pulmonary artery). LA: left atrium; LV: left ventricle; RV: right ventricle.
