Submitral aneurysm of the left ventricle (LV) is a rarely reported cardiac entity that can have a varied etiology. Primarily postulated to be caused by a congenital defect in the mitral annulus, secondary causes such as ischemic, rheumatic heart disease, infective and connective tissue disorders have also been described. We report a rare case of submitral aneurysm caused by tuberculous infestation of the mitral valve.
A 28-year-old man had a history of painless cervical lymphadenopathy and loss of appetite for six months. Fine needle-aspiration cytology of the cervical lymph node showed low yield mycobacterium tuberculosis (MTB) detected by Gene-Xpert. Anti-tuberculous therapy (ATT) was started by the treating physician, but the patient discontinued after one week. Subsequently, he reported orthopnea, exertional dyspnea and palpitation over the previous three months. He developed shortness of breath at rest, one day prior to admission.
On examination, he had reduced air entry on the right side with bilateral basal crepitations. Cardiac evaluation showed LVS3, 3/6 pan-systolic murmur at the mitral area. Diagnostic pleural fluid work-up revealed straw-colored fluid, 90 cells/high-power-field (95% lymphocytes, 5% polymorphs). The cartridge based nucleic acid amplification test of pleural fluid for MTB and blood culture were negative.
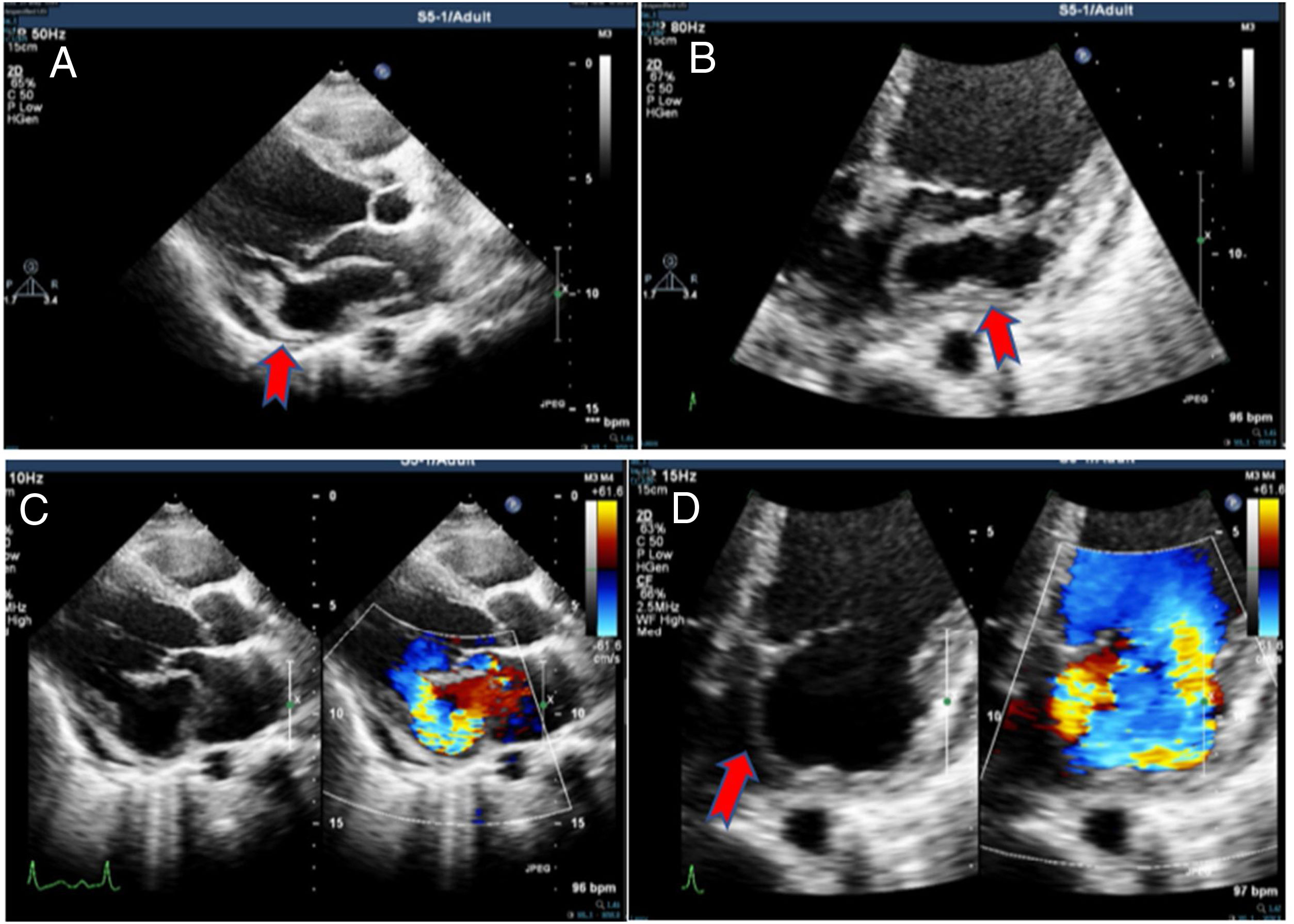
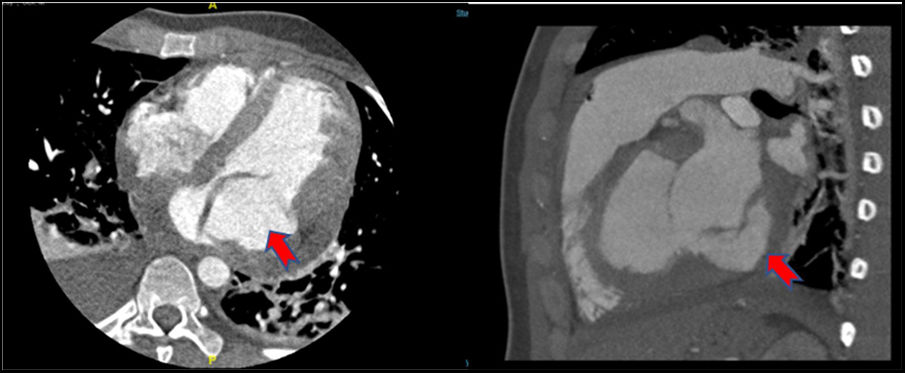
Echocardiographic evaluation (Figure 1) demonstrated posterior mitral leaflet (PML) prolapse with thick-walled aneurysm in the submitral area; cavity size 5.1 × 4.0 cm with to and fro flow into the cavity, with severe mitral regurgitation (MR), no vegetation and thin rim of pericardial effusion. Cardiac contrast-enhanced CT-scan (CECT) (Figure 2) also showed aneurysmal dilatation at the base of the LV along the mitral annulus with prolapse of PML into the left atrium (LA). Both LA and LV were dilated.
 and (C) (with colour Doppler) and AP4-chamber view (B) and (D) (with colour Doppler) showing aneurysm in the submitral area (red arrow) with to and fro flow into the cavity, with severe mitral regurgitation.")
 of the base of left ventricle along the mitral annulus with prolapse of posterior mitral leaflet into left atrium.")
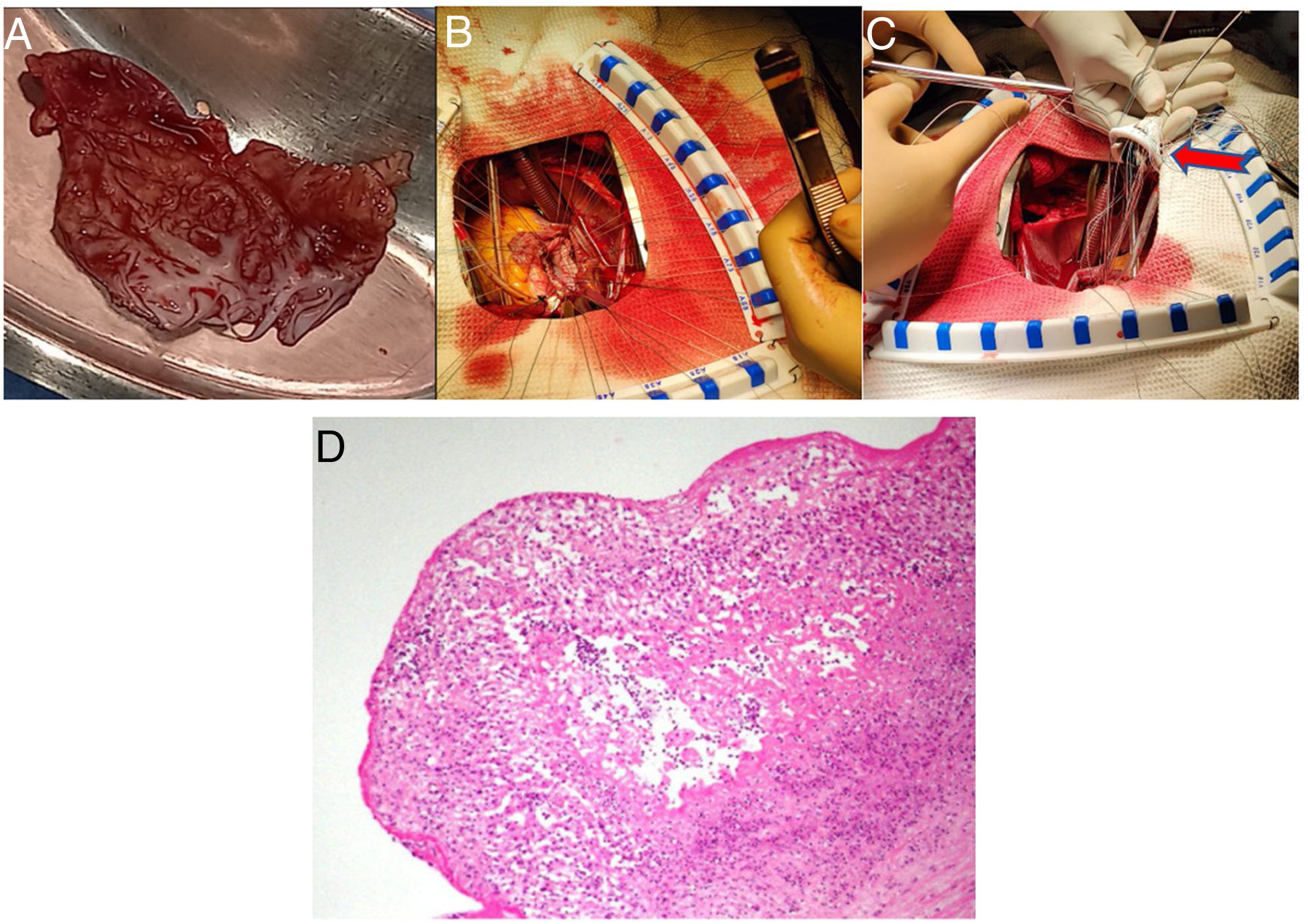
The patient was started on heart failure management. He was re-initiated on ATT and underwent early mitral annular reconstruction with a tanned pericardial patch and MV replacement with #25/33 mm On-X mechanical prosthetic valve (Figure 3A–C). Valve tissue on histopathological examination displayed necrotizing epithelioid cell granulomatous valvulitis (Figure 3D) along with the growth of acid fast bacilli in culture, suggestive of tuberculous etiology. The patient had an uneventful postoperative recovery and is currently on ATT and oral anticoagulation and doing well.
, mitral annular reconstruction (B) and On-X mechanical prosthetic valve (red arrow) implantation (C), histopathological examination of aneurysm specimen showing necrotizing epithelioid cell granulomas with giant cells (D).")
Intraoperative image showing the excised submitral aneurysm specimen (A), mitral annular reconstruction (B) and On-X mechanical prosthetic valve (red arrow) implantation (C), histopathological examination of aneurysm specimen showing necrotizing epithelioid cell granulomas with giant cells (D).
Submitral aneurysm or postero-basal aneurysm is an unusual cardiac condition first described by Abrahams et al. in patients of African origin.1 Congenital weakening in the posterior section of the mitral fibrous annulus or a disjunction between the LV and LA muscles are two potential etiologies.2 Infective diseases such as tuberculosis can very rarely lead to the development of submitral aneurysms, as in our case. Similar cases of tuberculous submitral aneurysm, in which patients developed heart failure and succumbed following surgery have been reported rarely.3,4 Presentation may be variable, small aneurysms are asymptomatic,2 larger ones present with dyspnea caused by MR secondary to imperfect coaptation of the leaflets, as in our patient. They can also present with life-threatening ventricular arrhythmias, thromboembolic phenomena, compression of a coronary artery, heart failure, rupture leading to death.4 Echocardiography and CECT are essential modalities for diagnosis.5 Early surgery is indicated in severe cases. Histopathological examination after surgery clinched the etiology as tuberculous in our patient. Proper compliance with anti-tuberculous medication must be ensured in these cases.
Patient consentConsent was obtained from the patient for the purpose of anonymized publication.
FundingNone declared.
Conflicts of interestThe authors declare that there is no conflict of interest.
We acknowledge the contributions of Department of Cardio-Thoracic surgery, SCTIMST Trivandrum for the surgical management of the case and for providing us with surgical and specimen images.
