








Training school children may help to increase the rate of citizen-initiated resuscitation. However, training in school settings exclusively by healthcare professionals would lead to high costs for the Portuguese National Health Service. The aim of this study was to assess the costs and effectiveness of training by school teachers, in comparison with training provided by healthcare professionals.
MethodsA quasi-experimental study was performed, with assessments before, immediately after, and two and a half months after the intervention. The costs and effectiveness of the training were compared in a sample of 362 students from the 10th, 11th and 12th grades, when performed by school teachers (experimental) versus health professionals (control).
ResultsRegarding knowledge retention and chest compressions, there was no significant difference between the groups two and a half months later. Regarding practical skills, the experimental group had improved more at two and a half months than the control group. However, no statistically significant differences were observed between the groups using multivariate analysis. The implementation and annual maintenance costs were 4043 and 862 euros, respectively, in the experimental group, and 8561 and 6430 euros in the control group.
Discussion and ConclusionsThe training provided by school teachers presented similar levels of effectiveness obtained at a lower cost, compared to the same training led by health professionals. This result suggests that generalizing training performed by school teachers could be valuable.
O treino em crianças escolarizadas pode contribuir para aumentar a taxa de reanimação iniciada pelo cidadão. No entanto, o treino generalizado em meio escolar, por profissionais de saúde, pode gerar custos elevados para o Serviço Nacional de Saúde. Este estudo procurou avaliar o custo e a efetividade do treino realizado por professores de ensino, em comparação com o treino realizado por profissionais da saúde.
MetodologiaFoi realizado um estudo quasi-experimental com avaliação inicial, imediatamente após a intervenção e dois meses e meio depois da mesma. Foram comparados os custos do programa e a efetividade do treino numa amostra de 362 crianças entre o 10.°, 11.° e 12.° ano, comparando o treino realizado por professores (experimental) e profissionais de saúde (controlo).
ResultadosNa retenção do conhecimento e na realização de compressões torácicas, não se encontraram diferenças significativas entre os grupos ao fim de dois meses e meio. Na demonstração de habilidades práticas, o grupo experimental melhorou mais aos dois meses e meio, em relação ao grupo controlo, face ao treino inicial. No entanto, na análise multivariada, não foram observadas diferenças estatisticamente significativas entre grupos. Os custos de implementação e manutenção (anuais) foram de 4043 e 862 euros respetivamente no grupo experimental, para 8561 e 6430 euros no grupo controlo.
Discussão e conclusõesO treino realizado por professores de ensino, apresenta níveis semelhantes de efetividade, obtidos com um custo mais baixo, que a mesma formação liderada pelos profissionais da saúde. Este resultado sugere o interesse da generalização do programa conduzido pelos professores.
Although mortality in Portugal associated with diseases of the circulatory system has fallen in recent years, mortality from ischemic heart disease has not, and in fact premature death from this cause has increased.1 The Portuguese National Program for Cerebrovascular Disease states that a large proportion of such deaths are classified as ‘sudden death’, which frequently occurs in out-of-hospital settings. Data from the Portuguese National Registry of Pre-Hospital Cardiac Arrest show that the most common location of cardiac arrest (CA) is the home, accounting for over 70% of CAs annually. CA was witnessed in around 35% of cases in these registries and the presumed cause was cardiac in over 50%.2
The treatment of CA involves a series of interlinked and standardized actions that make up the so-called ‘chain of survival’, which, when performed in an appropriate manner, lead to a substantial reduction in mortality due to CA.3 Citizens who witness an out-of-hospital CA can play an extremely important role by activating the medical emergency system and rapidly beginning cardiopulmonary resuscitation (CPR) maneuvers.4 However, lay bystanders usually have difficulty in identifying CA: not being familiar with the problem, they do not attempt to check vital signs, they confuse agonal breathing with normal respiration, and detection of CA is often delayed due to the unpredictability of sudden collapse and the range of different features that accompany the event.5 Lack of confidence during resuscitation, fear of litigation, and concerns about the risk of catching a disease during mouth-to-mouth ventilation are additional reasons for not undertaking CPR.6
Training of school children in CPR has been proposed as a valid way to increase the rate of bystander CPR.7,8 Efforts to this end by various organizations involved in resuscitation culminated in the approval by the World Health Organization in 2015 of programs to teach basic life support (BLS) in schools.9
It should be noted that having such programs taught by health professionals would be difficult to implement on a large scale in Portugal, given the current scarcity of resources available to the National Health Service. Although the curriculum of Physical Education classes in the 10th grade includes provision of first aid to victims of CA,10 no examples of actions aimed at providing students with this skill have been identified.
Against this background, the possibility has been raised of ‘training the trainers’, i.e. high school teachers, providing them with a tool that could be used to train all their classes in CPR without needing to involve health professionals after the initial training. However, it is not clear whether school teachers are as effective as health professionals in training students, or even if they are, that this effectiveness would be associated with efficient use of resources.
The aim of this study was to compare the effectiveness and costs of a program to train students in resuscitation maneuvers to be administered by school teachers with training provided by healthcare professionals.
MethodsStudy designThis was a quasi-experimental longitudinal prospective study, with assessments before, immediately after, and two and a half months after the intervention.
ParticipantsStudents (n=1405) were recruited from the 10th, 11th and 12th grades at the Mem Martins High School in the municipality of Sintra (Figure 1). Of these, 540 students (38.43%) were excluded because they were not enrolled in the Physical Education discipline, 481 students (34.23%) in 19 classes because their schedule did not allow time to participate in the study, 21 (1.5%) who took part in the pre-test to validate the data collection instrument, and one student (0.07%) who refused to give informed consent for participation.
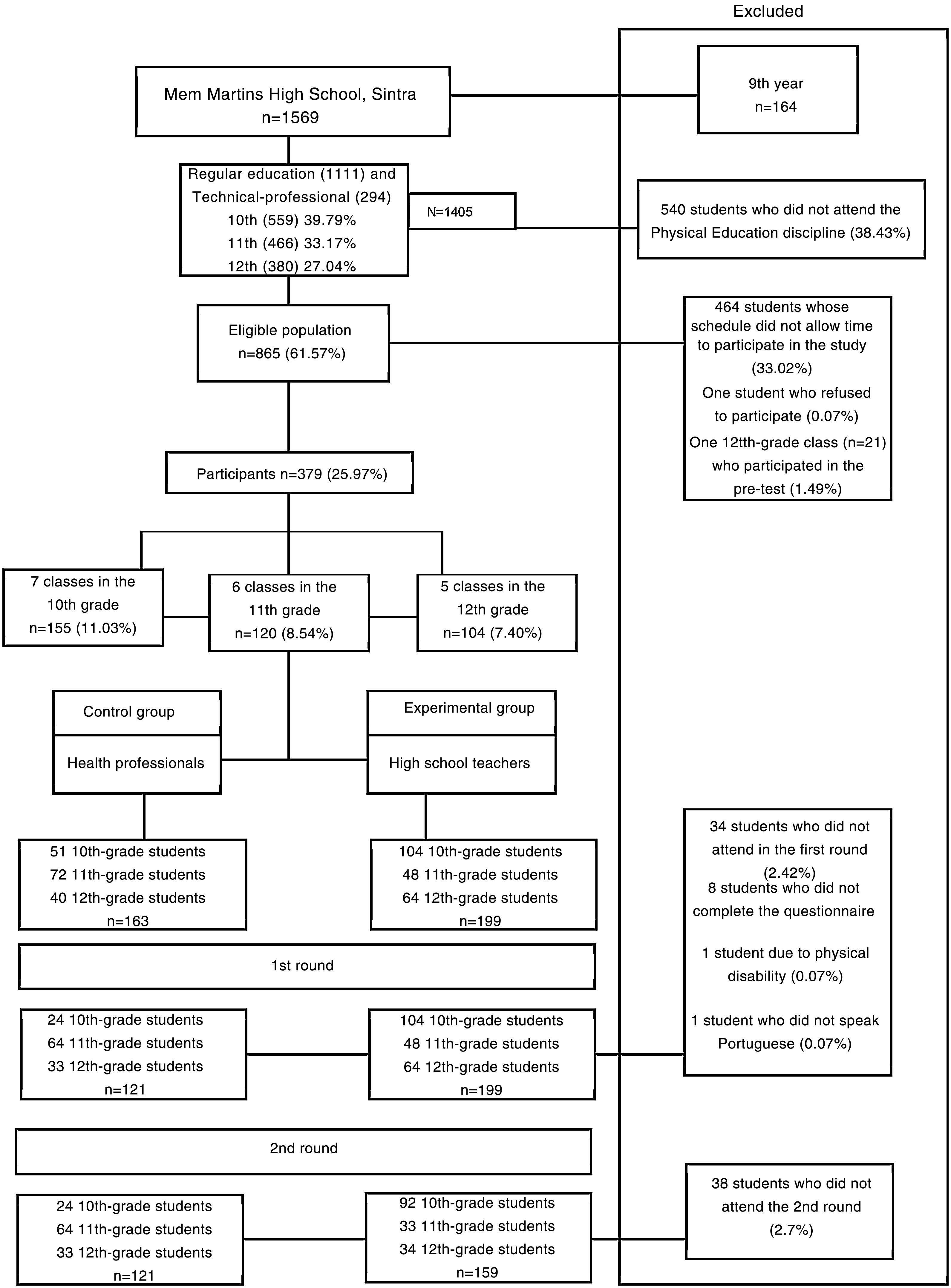
Random sampling of the classes led to the selection of 155 students in seven classes in the 10th grade (11.03%), 120 students in six classes in the 11th grade (8.54%), and 104 students in five classes in the 12th grade (7.40%), for a total of 379 school children. In the first round, 34 students who failed to attend, eight who did not complete Item B after training, one who did not speak Portuguese, and one who was physically unable to perform chest compressions on the manikin, were excluded. In the second round 38 students were excluded due to failure to attend.
The experimental group was composed of teachers from the high school, while the control group consisted of health professionals, all of them nurses or physicians from Hospital Professor Doutor Fernando da Fonseca, Amadora (HFF). All instructors had taken the Basic Life Support and Automated External Defibrillator (BLS+AED) course certified by the American Heart Association and the Portuguese National Institute for Emergency Medicine (INEM) and the instructors’ course in “Aprende os 3C's – Salva uma vida” (Learn the Three Cs – Save a Life), a training program for instructors in schools (Appendix 1). The level of practical skills achieved was assessed by the instructors themselves under the supervision of the lead investigator of the study.
InterventionField work for the study took up two class periods. It was performed in the school itself and was divided into two rounds. The first round took place in morning and afternoon periods between March 11 and 20, 2019, while the second round (reassessment) took place in the same class periods between May 27 and 31. Based on information provided by the school's Executive Board on the composition of the classes, a ratio of up to 15 students per instructor was assumed.
The instrument used to evaluate the effectiveness of the simulated practice (Appendix 2) consisted of four items:
Item A: sociodemographic characterization of the study sample;
Item B: assessment of the student's previous knowledge about CA as presented in the video (see below), to be filled in individually under the instructor's supervision, consisting of 10 questions with responses scored between 0 and 1011;
Item C: practical case in which students demonstrate specifically how to implement safety measures, identify a CA, call the emergency number (112) and communicate appropriately, and place their hands on the victim's chest (between 5 and 20 points for each section, for a maximum score of 100)12;
Item D: chest compressions on a manikin for 2 min, performed by students individually, supervised and recorded by the instructor. International guidelines recommend a rate of 100-120 compressions/min and a depth of approximately 5 cm. The compressions were counted manually with the help of a smartphone app. A Laerdal Mini Anne Plus® manikin13 was used.
The instrument was reviewed by two school teachers and seven students with similar characteristics to the study sample, who suggested changes to the text. Items B and C were validated by one physician and four nurses, all experts in emergency medicine and trainers on PCR courses (Appendix 3). A pre-test was carried out with 21 students in the 12th grade at the same school.
In the first round, all participants were given around 15 min to complete a test assessing their previous knowledge about CA (Items A and B), and then attended a training session in which they watched a 16-min video. The practical case was then applied (Items C and D), taking around 5 min for each participant. The participants then responded to another assessment of their knowledge with the same questions (Item B). In the second round two and a half months later, a reassessment took place (without watching the video) that included the practical case (Items C and D) and assessment of post-training knowledge retention (Item B). The entire course of the intervention is summarized in Figure 2.
Calculation of costs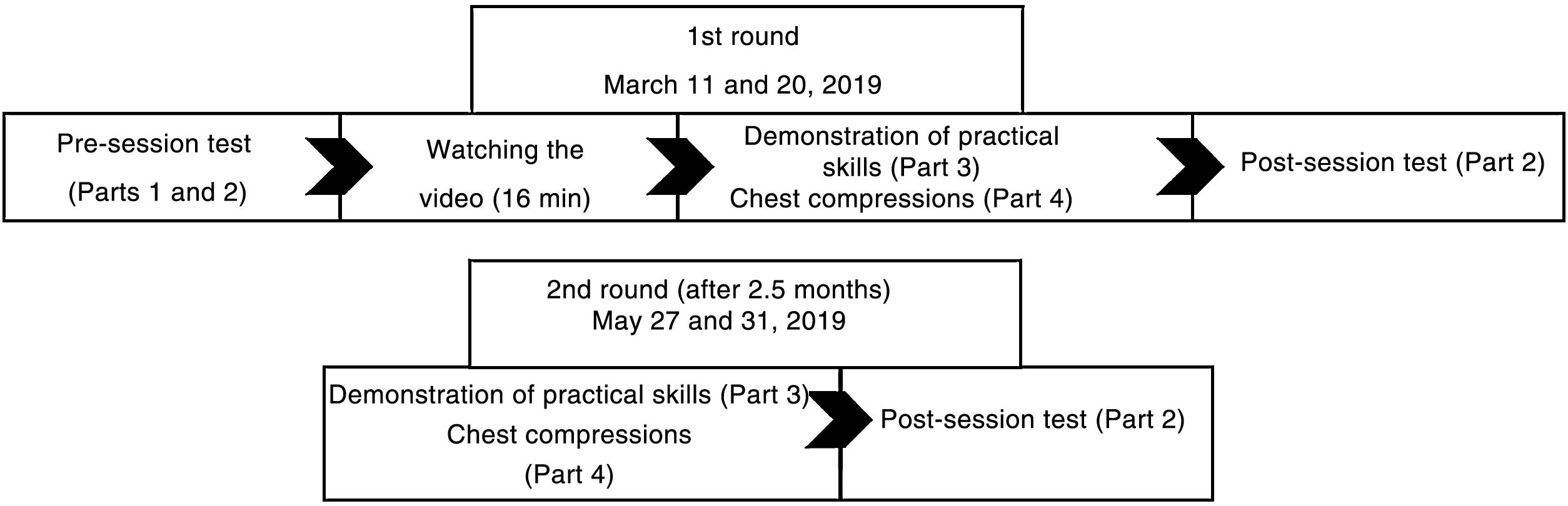
The costs of implementing and maintaining the training program were estimated based on data provided by Sintra Town Hall, the Resuscitation School of HFF, and current legislation. Information was collected on:
- (a)
costs of certified training in BLS+AED for the experimental and control groups;
- (b)
costs of training sessions delivered by the control group, since these took place outside normal working hours;
- (c)
costs of initial preparation of school teachers and regular annual visits for quality control of the program. Costs of the training and initial preparation sessions were calculated on the basis of the standard rates used in the Resuscitation School for remuneration of instructors;
- (d)
cost of acquiring the Laerdal Mini Anne Plus® manikins (2018 prices);
- (e)
traveling expenses;
- (f)
costs of online data storage on a cloud hosting service.
These costs were extrapolated to cover all students in the 10th, 11th and 12th grades at the school (n=1405).
Calculation of effectiveness: univariate analysisA non-parametric median test was used to compare the medians of continuous variables in the experimental and control groups, in order to assess the quality of the randomization and to identify possible sources of bias. The chi-square test was used to compare categorical variables.
Calculation of effectiveness: multivariate analysisA general linear model was applied to determine whether the differences in effectiveness between the experimental and control groups were statistically significant, adjusting for variables with significant differences between the groups on univariate analysis. This adjustment was designed to avoid measurement bias when calculating the impact of the intervention arising from the fact that the characteristics of the adjustment were not necessarily similar between the two groups.
The significance level was taken to be 5% (p-value <0.05).
Ethical considerationsThe study was authorized by the Clinical Research Unit and the Resuscitation School of HFF, the ethics committee of the NOVA Medical School of Universidade Nova, Lisbon, the Directorate-General for Education (case no. 0665400001), and the Executive Board of the school group in which the study took place. Informed consent was requested from parents or guardians and students were asked if they were willing to participate. All data collected were anonymized and consent was deemed to be passive, i.e. the consent form was filled and signed only in cases of refusal, with failure to respond being considered equivalent to consent.
ResultsUnivariate analysisItem A: characterization of the study populationMean age in the experimental group (n=186) was 16 years, compared to 17 years in the control group (n=132) (p<0.084). There were statistically significant differences between the groups in mean grades in the previous year, the ways that students related to each other and to the school, and the closeness of students to people in the school (Table 1).
Characteristics of the study population.
| Continuous variables | E | C | p |
|---|---|---|---|
| Age, years (median) | 16 | 17 | 0.084a |
| Categorical variables | E, % | C, % | p |
| Male gender | 40.9 | 48.5 | 0.177b |
| Distribution by school year | |||
| 10th grade | 55.9 | 18.2 | <0.001b |
| 11th grade | 18.3 | 51.5 | |
| 12th grade | 25.8 | 30.3 | |
| Grades in previous year (maximum 20) | |||
| <10 | 10.1 | 3.0 | 0.007b |
| 10-13 | 44.9 | 62.1 | |
| 14-16 | 40.4 | 29.5 | |
| 17-18 | 3.9 | 3.0 | |
| 19-20 | 0.6 | 2.3 | |
| Self-perception of state of health | |||
| Excellent | 20.7 | 23.7 | 0.412b |
| Good | 64.7 | 57.3 | |
| Reasonable | 14.1 | 19.1 | |
| Poor | 0.5 | 0 | |
| Mother's education level | |||
| Completed basic education or less | 20.4 | 21.5 | 0.479b |
| Did not complete high school | 11.0 | 15.4 | |
| Completed high school | 34.3 | 30.0 | |
| Did not complete higher education | 6.1 | 5.4 | |
| Completed higher education | 19.9 | 23.8 | |
| Don’t know | 8.3 | 3.8 | |
| Father's education level | |||
| Completed basic education or less | 26.0 | 27.5 | 0.469b |
| Did not complete high school | 13.3 | 18.3 | |
| Completed high school | 29.3 | 25.2 | |
| Did not complete higher education | 5.0 | 1.5 | |
| Completed higher education | 14.9 | 16.8 | |
| Don’t know | 11.6 | 10.7 | |
| Previous BLS training | |||
| Yes | 74.6 | 80.8 | 0.199b |
| No | 25.4 | 19.2 | |
| Relatives with knowledge of BLS, % | |||
| Father | 12.3 | 13.9 | 0.771b |
| Mother | 19.9 | 16.4 | |
| Sibling | 6.4 | 9 | |
| Aunt or uncle | 10.5 | 9.8 | |
| None | 35.7 | 32.8 | |
| Relatives with heart disease | |||
| Yes | 36.7 | 25.2 | 0.794b |
| No | 53.1 | 65.5 | |
| Don’t know | 9.4 | 9.2 | |
| Student's relationship with other students and with the school | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Disagree completely, % | Disagree, % | Agree, % | Agree completely, % | p | |||||
| E | C | E | C | E | C | E | C | ||
| I feel close to the people in my school | 2.2 | 9.2 | 18.9 | 23.7 | 66.5 | 59.5 | 12.4 | 7.6 | 0.015b |
| I feel part of my school | 1.6 | 5.4 | 9.8 | 13.1 | 72.8 | 64.6 | 15.8 | 16.9 | 0.178b |
| I am happy to be in my school | 2.7 | 3.8 | 11.3 | 14.6 | 69.4 | 71.5 | 16.7 | 10 | 0.322b |
| I feel that the teachers in my school treat me fairly | 1.1 | 2.3 | 11.3 | 13.7 | 69.9 | 70.2 | 17.7 | 17.7 | 0.602b |
| I feel safe in my school | 2.2 | 3.1 | 4.3 | 11.5 | 69.4 | 67.9 | 24.2 | 17.6 | 0.064b |
The median score obtained in the assessment of knowledge of CA was 6.00 in both the experimental and the control group (p=0.928). Immediately after the training session, the median score increased to 9.00 in both groups (p=0.227), while after 2.5 months the median improvement was slightly greater in the control group, but without statistical significance (Table 2).
Results of simulated training.
| Continuous variables | E | C | pa | ||
|---|---|---|---|---|---|
| Median | IQR | Median | IQR | ||
| Test of knowledge | |||||
| Pre-test score | 6.0 | 2.0 | 6.0 | 2.0 | 0.928a |
| Post-test score | 9.0 | 1.0 | 9 | 1.0 | 0.227a |
| Score at 2.5 months | 9.0 | 1.0 | 9 | 1.0 | 0.568a |
| Difference between total post-session score and total pre-session score | 2.0 | 2.0 | 3 | 2.0 | <0.001a |
| Difference between total score after 2.5 months and total pre-session score | 2.5 | 2.0 | 2.0 | 1.5 | <0.001a |
| Variance in the differences between total post-session score and total pre-session score | 0.111a | ||||
| Variance in the differences between total score after 2.5 months and total pre-test score | 0.933a | ||||
| Test of practical skills | |||||
| Total score for practical skills in the 1st round (immediately after watching the video) | 80.0 | 30.0 | 80.0 | 25.0 | 0.455a |
| Total score for practical skills in the 2nd round (2.5 months later) | 85.0 | 25.0 | 75.0 | 20.0 | 0.001a |
| Difference between total score for practical skills in the 2nd round and total score for practical skills in the 1st round | 5.0 | 25.0 | 0.0 | 30 | E: 0.008a |
| C: 0.038a | |||||
| Variance in the differences between total score for practical skills in the 2nd round and total score for practical skills in the 1st round | 0.006a | ||||
| Test of psychomotor performance | |||||
| Frequency of chest compressions (2 min) in the 1st round | 226.0 | 66.0 | 222.0 | 53.0 | 0.430a |
| Frequency of chest compressions in the 2nd round | 218.0 | 65.0 | 226.0 | 50.0 | 0.339a |
| Categorical variables | E, % | C, % | pb | ||
| Test of psychomotor performance according to the guidelines (200-240 chest compressions in 2 min) | |||||
| Frequency of chest compressions (2 min) in the 1st round outside recommended range | 68.8 | 59.1 | 0.074b | ||
| Frequency of chest compressions (2 min) in the 1st round within recommended range | 31.2 | 40.9 | |||
| Frequency of chest compressions (2 min) in the 2nd round outside recommended range | 66.1 | 58.3 | 0.156b | ||
| Frequency of chest compressions (2 min) in the 2nd round outside recommended range | 66.1 | 58.3 | 0.156b | ||
| Frequency of chest compressions (2 min) in the 2nd round within recommended range | 33.9 | 41.7 | |||
After students watched the video in the first round, their median score did not differ significantly between the groups (p=0.455). In the second round the performance of the experimental group was better, with a statistically significant difference (p=0.001). There were statistically significant improvements in both the experimental (p=0.008) and the control group (p=0.038) (Table 2).
Item D: chest compressionsIn the first round, 31.2% of participants in the experimental group and 40.9% of the control group performed chest compressions within the recommended range (p=0.074) (Table 2). In the second round, these figures rose to 33.9% in the experimental group and 41.7% in the control group (p=0.156) (Table 2).
Multivariate analysisIn the calculation of effectiveness, multivariate analysis was used to adjust for dimensions in which significant differences had been observed in univariate analysis. Specific adjustments were made for school year, grades in the previous year, and the student's relationship with the school. A log-normal distribution was assumed for the three dependent variables, as the distributions had been shown to be non-normal.
Multivariate analysis showed that improvements in knowledge retention immediately after the training session and 2.5 months later (Item B) did not differ significantly between the experimental and control groups. The greater improvement in practical skills (Item C) observed in the experimental group was also confirmed but again without statistical significance. Finally, regarding chest compressions (Item D), there were greater improvements in the control group, although once more without statistical significance (Table 3).
Multivariate analysis adjusting for variables with statistical significance in univariate analysis (school year, grades in previous year, and relationship with the school).
| Dependent variables | Experimental group (vs. control) | ||
|---|---|---|---|
| Coefficient | Standard error | p | |
| Difference in pre-test vs. post-test (Item B) | -0.150 | 0.081 | 0.066 |
| Difference in pre-test vs. 2.5 months later (Item B) | -0.122 | 0.089 | 0.167 |
| Difference in practical skills before vs. 2.5 months later (Item C) | 0.725 | 0.624 | 0.245 |
| Difference in chest compressions before vs. 2.5 months later (Item D) | 13.81 | 647.291 | 0.983 |
Costs arising from the training program were lower in the experimental group than in the control group. The costs of implementing and maintaining the program, extrapolated for all students of the 10th, 11th and 12th grades in the following year, were 4043 and 862 euros, respectively, in the experimental group, and 8561 and 6430 euros in the control group.
If the program had been implemented as in the control group only, the costs extrapolated to the year of implementation would be 8561 euros, falling to 6430 euros in the following year.
The item with the greatest cost was the Aprende os 3C's series of training sessions (6000 euros), which would account for 70.1% of the total cost in the year of implementation and 93.3% in the following year.
If the program had been delivered as in the experimental group, the main costs in the year of implementation would have been (a) training the school teachers in BLS+AED and Aprende os 3C's, with 1113 euros (27.5% of the total cost) and 120 euros (3.0% of the total cost), respectively; (b) acquisition of the training manikins, with 1426 euros (35.3% of the total cost); and (c) initial preparation and quality audit of the session, a total of 1200 euros (29.7% of the total cost). However, in the following year, the quality audit of the session by itself would incur the highest cost, with 600 euros (69.6% of the total cost). Costs of implementation are higher than maintenance costs in both groups (Table 4).
Distribution of costs (in euros) by group and by year.
| Resource | Control group | ||||||
|---|---|---|---|---|---|---|---|
| Implementation (1st year) | 2nd and 3rd years | ||||||
| Unit cost | Quantity | Total | Quantity | Total | Source | ||
| Certified BLS+AED course (clinical) | 70.50 | Trainee | 10 | 705.00 | 0 | 0 | ERHFF |
| Training in Aprende os 3C's | 120.00 | Course | 1 | 120.00 | 1 | 120.00 | ERHFF |
| Training manikins | 713.00 | Box | 2 | 1426.00 | 0 | 0 | CMS |
| Training session in Aprende os 3C's at the school | 120.00 | Session | 50 | 6000.00 | 50 | 6000.00 | ERHFF |
| Travel between hospital and school | 0.40 | km | 525 | 210.00 | 525 | 210.00 | Legislation |
| Quality audit of the session | 120.00 | Audit | 0 | 0 | 0 | 0 | ERHFF |
| Cloud data storage | 100.00 | Record | 1 | 100.00 | 1 | 100.00 | Dropbox |
| Initial preparation | 120.00 | Session | 0 | 0 | 0 | 0 | ERHFF |
| Total | 8561.00 | 6430.00 | |||||
| Cost per student (n=1405) | 6.1 | 4.58 | |||||
| Resource | Experimental group | ||||||
|---|---|---|---|---|---|---|---|
| Implementation (1st year) | 2nd and 3rd years | ||||||
| Unit cost | Quantity | Total | Quantity | Total | Source | ||
| Certified BLS+AED course (non-clinical) | 111.30 | Trainee | 10 | 1113.00 | 0 | 0 | CMS |
| Training in Aprende os 3C's | 120.00 | Course | 1 | 120.00 | 1 | 120.00 | ERHFF |
| Training manikins | 713.00 | Box | 2 | 1426.00 | 0 | 0 | CMS |
| Travel between hospital and school | 0.40 | km | 210 | 84.00 | 105 | 42.00 | Legislation |
| Quality audit of the session | 120.00 | Audit | 5 | 600.00 | 5 | 600.00 | ERHFF |
| Cloud data storage | 100.00 | Record | 1 | 100.00 | 1 | 100.00 | Dropbox |
| Initial preparation | 120.00 | Session | 5 | 600.00 | 0 | 0 | ERHFF |
| Total | 4043.00 | 862.00 | |||||
| Cost per student (n=1405) | 2.88 | 0.61 | |||||
BLS+AED: basic life support and automated external defibrillator; CMS: Sintra Town Hall; ERHFF: Resuscitation School of Hospital Professor Doutor Fernando Fonseca; Legislation: Implementing Order no. 1553-D/2008 amended by Decree-Law no. 137/2010.
On multivariate analysis, there were no statistically significant differences between the experimental and control groups with regard to knowledge retention (Item B), demonstration of practical skills (Item C), or performing chest compressions (Item D), either in the initial period or after 2.5 months or in the difference between the two periods. The multivariate analysis enabled adjustment of the comparison between groups for possible confounding factors, including bias due to differences in the characteristics of the two groups. In terms of magnitude of the effect, without adjustment there was an improvement in the practical skills of the experimental group, while gains were greater in the control group for knowledge retention and chest compressions.
The costs of the program were lower when it was delivered by the experimental group, with savings of 4500-5500 euros, depending on the need to acquire training resources or material in other years.
Interpretation of the resultsThe main result is that when adjusted for differences between the groups, no differences in the effectiveness of the intervention were seen between health professionals and school teachers. This is to be expected regarding practical skills and chest compressions, since these are taught in part through the same video.11 Furthermore, the greater technical knowledge of the health professionals could be balanced by the closer relationship between the school teachers and their students, by their experience in transmitting knowledge, and by their greater ability to adapt their language for a young audience, especially when they have been trained in BSL+AED.14
Other points deserve mention with regard to effectiveness. For Item B, other studies have observed statistically significant improvements in knowledge retention before training, immediately after, and at two and four months,11,12 as we found in univariate analysis. There is a reference in the literature to a decline in knowledge retention after six months, although assessment of this variable was not within the scope of our study. Annual training sessions may lead to better results, as well as being easier to integrate into school curricula and improving use of the school's resources.12
An unexpected result was the low effectiveness of training in frequency of chest compressions (Item D). International guidelines recommend a frequency of 100-120/min, with a depth of approximately 5 cm but not exceeding 6 cm, allowing full chest recoil after each compression, maintaining an equal time between compression and recoil, and minimizing interruptions.15 However, around 70% of participants in the experimental group and 60% in the control group did not achieve the recommended rate of chest compressions (100-120/min). We recognize the need to improve training in this respect in future applications of the program.
Analysis of costsAccording to a study by Lockey et al., the British Heart Foundation estimated the cost of implementing its Heartstart program to be 2100 GBP.16 This includes the cost of the training manikins, audiovisual educational aids, and the instructor who carries out the training sessions. Maintenance costs include those for replacing manikins and consumables, and instructor costs. Lockey et al. do not specify the type of instructor or number of students covered by the Heartstart program, or whether the training of instructors is certified. These variables may explain the lower costs they calculated compared to the results of our study.
Calculation of costs in the present study was based on estimates and retrospective analysis. Costs were extrapolated to the entire school, since all students in the 10th, 11th and 12th grades would be covered by the training. The highest cost was attributed to training sessions in the school when the program was delivered only by health professionals, in which case the sessions took place outside normal working hours. Payments for these sessions were calculated at the rate stipulated by the Resuscitation School for their instructors. If the sessions had taken place during normal working hours, payments would have been adjusted to the contracted price per hour for the instructor's professional category. However, this would entail these health professionals being unable to perform their usual duties during these hours. The hours of the school teachers, who delivered the training as part of their normal activity, were costed according to the contracted price per hour for their professional category. The training sessions took up two class periods as part of the core curriculum of the Physical Education discipline for 10th-year students, and so the teacher did not require additional time to prepare the lessons.
Other authors have compared conventional training techniques (with health professionals, school teachers, videos and manikins) with other low-cost training techniques such as foam dice, videos, and peer instruction by fellow students,17,18 but it would be difficult to compare their results with ours.
LimitationsFirstly, the time between the two training sessions was 2.5 months, whereas the shortest interval found in the literature was thee months. However, the difference was only 15 days relative to the best evidence, and was the same for both groups, and so we consider that this limitation would have had little effect. Secondly, the study analyzed only one school. The results may therefore not be applicable to other groups and may not reflect the situation in the country as a whole. In particular, the population of the catchment area of the hospital (Amadora and Sintra municipalities) is in general underprivileged, with low education levels and income,19,20 which may mean that the intervention was less effective than it would have been in other parts of the country. Nevertheless, the aim of this study was not only to assess its effectiveness in schools, but also to compare the effectiveness of two professional groups, health professionals and high school teachers.
ConclusionsThe present study shows that a training program in resuscitation maneuvers for high school students can be implemented by school teachers with similar levels of effectiveness to health professionals and at lower cost. It is a contribution to the preparation of strategic actions set out in the core curriculum of the Physical Education discipline for 10th-year students. We suggest that this is the best approach provided that conditions are suitable for its roll-out in other schools of this municipality and other regions of the country.
Conflicts of interestThe authors have no conflicts of interest to declare.
The following are the supplementary material to this article:

Description of the “Aprende os 3C's – Salva uma vida” (Learn the Three Cs – Save a Life) training program in resuscitation maneuvers.

Data collection instrument.

Expert panel responsible for validation of the data collection instrument.
